Download
1 / 1
10 likes | 90 Views
Poster 26473. Assessment of Low Resolution Detectors for Radiostereometry. Martin R. Downing, George P. Ashcroft. Aberdeen RSA Imaging Group, School of Medicine & Dentistry, University of Aberdeen, Scotland, UK. m.downing@abdn.ac.uk. Introduction

E N D
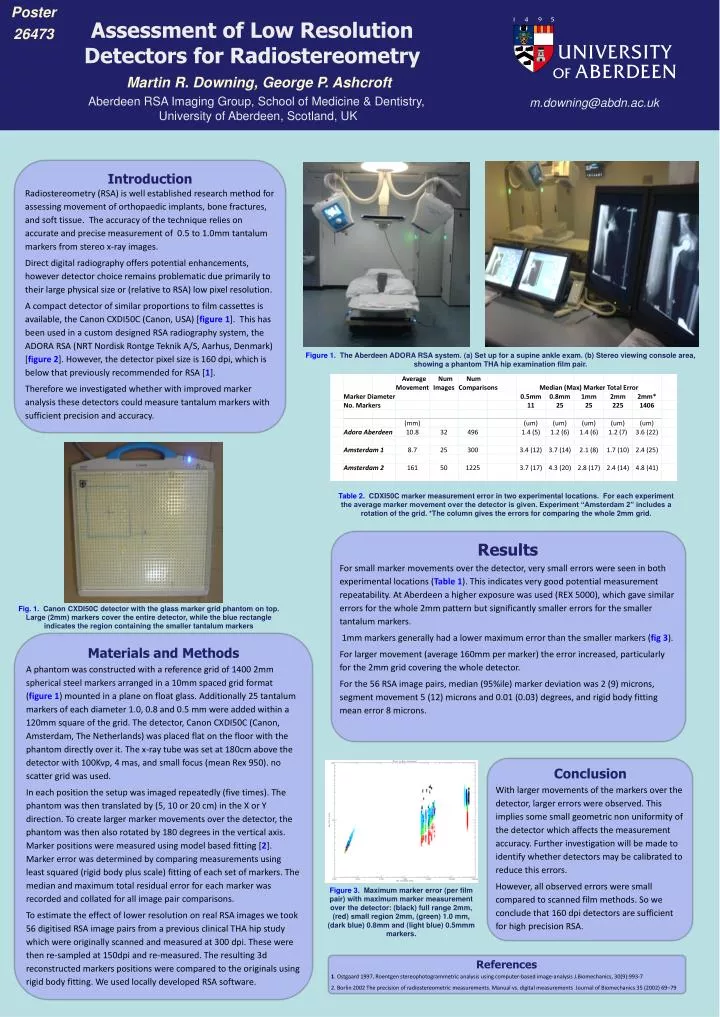
Poster 26473 Assessment of Low Resolution Detectors for Radiostereometry Martin R. Downing, George P. Ashcroft Aberdeen RSA Imaging Group, School of Medicine & Dentistry, University of Aberdeen, Scotland, UK m.downing@abdn.ac.uk Introduction Radiostereometry (RSA) is well established research method for assessing movement of orthopaedic implants, bone fractures, and soft tissue. The accuracy of the technique relies on accurate and precise measurement of 0.5 to 1.0mm tantalum markers from stereo x-ray images. Direct digital radiography offers potential enhancements, however detector choice remains problematic due primarily to their large physical size or (relative to RSA) low pixel resolution. A compact detector of similar proportions to film cassettes is available, the Canon CXDI50C (Canon, USA) [figure 1]. This has been used in a custom designed RSA radiography system, the ADORA RSA (NRT Nordisk RontgeTeknik A/S, Aarhus, Denmark) [figure 2]. However, the detector pixel size is 160 dpi, which is below that previously recommended for RSA [1]. Therefore we investigated whether with improved marker analysis these detectors could measure tantalum markers with sufficient precision and accuracy. Figure 1. The Aberdeen ADORA RSA system. (a) Set up for a supine ankle exam. (b) Stereo viewing console area, showing a phantom THA hip examination film pair. 4 7 Table 2. CDXI50C marker measurement error in two experimental locations. For each experiment the average marker movement over the detector is given. Experiment “Amsterdam 2” includes a rotation of the grid. *The column gives the errors for comparing the whole 2mm grid. Results For small marker movements over the detector, very small errors were seen in both experimental locations (Table 1). This indicates very good potential measurement repeatability. At Aberdeen a higher exposure was used (REX 5000), which gave similar errors for the whole 2mm pattern but significantly smaller errors for the smaller tantalum markers. 1mm markers generally had a lower maximum error than the smaller markers (fig 3). For larger movement (average 160mm per marker) the error increased, particularly for the 2mm grid covering the whole detector. For the 56 RSA image pairs, median (95%ile) marker deviation was 2 (9) microns, segment movement 5 (12) microns and 0.01 (0.03) degrees, and rigid body fitting mean error 8 microns. Fig. 1. Canon CXDI50C detector with the glass marker grid phantom on top. Large (2mm) markers cover the entire detector, while the blue rectangle indicates the region containing the smaller tantalum markers Materials and Methods A phantom was constructed with a reference grid of 1400 2mm spherical steel markers arranged in a 10mm spaced grid format (figure 1) mounted in a plane on float glass. Additionally 25 tantalum markers of each diameter 1.0, 0.8 and 0.5 mm were added within a 120mm square of the grid. The detector, Canon CXDI50C (Canon, Amsterdam, The Netherlands) was placed flat on the floor with the phantom directly over it. The x-ray tube was set at 180cm above the detector with 100Kvp, 4 mas, and small focus (mean Rex 950). no scatter grid was used. In each position the setup was imaged repeatedly (five times). The phantom was then translated by (5, 10 or 20 cm) in the X or Y direction. To create larger marker movements over the detector, the phantom was then also rotated by 180 degrees in the vertical axis. Marker positions were measured using model based fitting [2]. Marker error was determined by comparing measurements using least squared (rigid body plus scale) fitting of each set of markers. The median and maximum total residual error for each marker was recorded and collated for all image pair comparisons. To estimate the effect of lower resolution on real RSA images we took 56 digitised RSA image pairs from a previous clinical THA hip study which were originally scanned and measured at 300 dpi. These were then re-sampled at 150dpi and re-measured. The resulting 3d reconstructed markers positions were compared to the originals using rigid body fitting. We used locally developed RSA software. 5 8 Conclusion With larger movements of the markers over the detector, larger errors were observed. This implies some small geometric non uniformity of the detector which affects the measurement accuracy. Further investigation will be made to identify whether detectors may be calibrated to reduce this errors. However, all observed errors were small compared to scanned film methods. So we conclude that 160 dpi detectors are sufficient for high precision RSA. Figure 3. Maximum marker error (per film pair) with maximum marker measurement over the detector: (black) full range 2mm, (red) small region 2mm, (green) 1.0 mm, (dark blue) 0.8mm and (light blue) 0.5mmm markers. 3 6 9 References 1. Ostgaard 1997, Roentgen stereophotogrammetric analysis using computer-based image-analysis J.Biomechanics, 30(9):993-7 2. Borlin 2002 The precision of radiostereometric measurements. Manual vs. digital measurements Journal of Biomechanics 35 (2002) 69–79






