Download
1 / 39
400 likes | 644 Views
The History of Medicare: From Inception to Social Institution. MaCie Rogers Mercer University College of Pharmacy & Health Sciences Pharm.D Candidate 2013. Primarily adapted from: THE EVOLUTION OF MEDICARE . . . from idea to law by Peter A. Corning (1969).

E N D
The History of Medicare: From Inception to Social Institution MaCie Rogers Mercer University College of Pharmacy & Health Sciences Pharm.D Candidate 2013 Primarily adapted from: THE EVOLUTION OF MEDICARE . . . from idea to law by Peter A. Corning (1969)
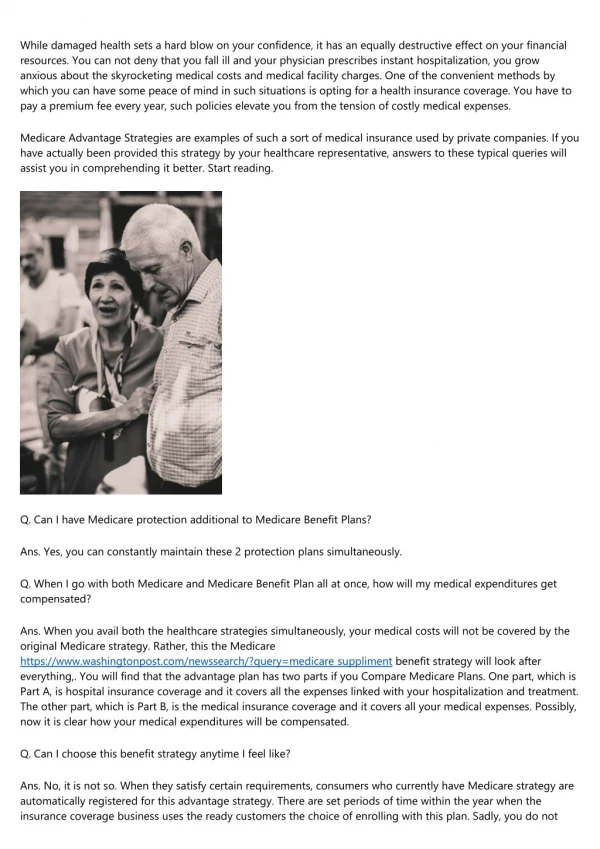
July 30, 1965: President Lyndon B. Johnson signs H.R. 6675 (Public Law 89-97) establishing Medicare for the elderly and Medicaid for the indigent Signed in Independence, MO in the presence of Harry S. Truman who advocated for such legislation in an address to congress in 1945. Former President Truman became the first to enroll in Medicare
Global Roots • Funeral societies of ancient Greece originated the idea and individuals pooling their resources in order to spread economic risks • Medieval craft guilds often set up welfare funds for the assistance of the sick and needy • Citizens of Greek city-states enjoyed tax-supported public physicians • 1758- US government set up the Marine Hospital Service, which required owners of merchant ships to contribute 20 cents/mth into a “sickness fund” for each seaman they employed; this was the origination of compulsory participation • 1854- The State of Prussia enacted the first broad-gauged compulsory health insurance law
The First Wave 1912-1920
The AALL • The movement for Government health insurance in the US was spearheaded by a group called the American Association for Labor Legislation (AALL), a private reform organization • The AALL’s first campaign was on behalf of State laws to require employers to insure their employees against industrial accidents- AKA workman’s compensation • By 1913, 30 states passed such laws • By 1916, there were congressional hearings on compulsory State-run health insurance
The Fight Continues • 1916-1917: The American Medical Association (AMA) Social Insurance Committee recommends compulsory, State-run health insurance and passes a resolution stating principles to be followed in Government health insurance plans • Oct 1917 : War Risk Insurance Act passed established a comprehensive system of benefits, including health insurance, for servicemen and their dependents • 1918: First Federal grants to States for public health services.
The Tide Turns • November 1918: California voters defeat a referendum to permit establishment of a State health insurance plan by a 2-to-1 margin • April 1919: New York State Assembly defeats a health insurance bill previously approved by the State Senate. • 1920: AMA House of Delegates reverses position, declaring itself in opposition to Government health insurance • Supporters of the movement went underground and did not re-surface until the late 1920’s
“Sickness is not a problem for the community as a whole" [and Government health insurance is not] "necessary, wise, or desirable." The National Association of Manufacturers' Committee on Industrial Betterment- 1917
The Second Wave 1927-1940
The Roaring 20’s: The “Seedtime of Reform” • The 1920’s in the United States was a time of decadence and excess to great disregard of social and political problems • Reform groups such as the National Consumers' League, the National Conference of Social Work, the National Child Labor Committee, the National Federation of Settlements, the American Association of Social Workers, and the American Association for Labor Legislation kept the idea of social welfare alive • 1921: Sheppard-Towner act enacted- provided Federal subsidies for State-run child and maternal health programs
The CCMC • The 2nd major organization to spearhead the fight for adequate healthcare financing was Committee on the Costs of Medical Care • Originally formed to conduct the Nation's first comprehensive study of medical economics, the CCMC produced a final report recommending vast changes to the financing and organization of health-care
CCMC Recommendations (ca. 1932) • Efforts to organize medical practice, with the hospital (preferably) rather than the solo medical practitioner, at the focal point • Extension of public health services • Group payment for medical care, either through taxation (along the lines of the present Medicaid program, through private health insurance, or both) • Large-scale planning and coordination of health services • Numerous changes in medical education, both for physicians and for allied professions such as nursing and pharmacy • Of note, the CCMC did not advocate a compulsory government health insurance system
The New Deal "One of the duties of the State is that of caring for those of its citizens who find themselves the victims of such adverse circumstances as makes them unable to obtain even the necessities for mere existence without the aid of others. That responsibility is recognized by every civilized nation. . . . To these unfortunate citizens aid must be extended by Government--not as a matter of charity but as a matter of social duty.“ ~ President Theodore Roosevelt
The New Deal • After his election in 1932, amidst The Great Depression, President Theodore Roosevelt introduced “The New Deal”, a plan for economic and social reform • Launched such agencies as Federal Emergency Relief Administration (FERA) , the Public Works Administration (PWA), the Civil Works Administration (CWA), the National Recovery Administration (NRA), and the Civilian Conservation Corps (CCC) • 1934: President Roosevelt established the “Committee on Economic Security” and instructed them to explore “all forms of social insurance” including Government-run health insurance
Considerations of Government health insurance were immediately met with opposition, primarily from physicians and other members of the medical profession • 1932 : American Federation of Labor (AFL) endorses social insurance • 1935: • January- Committee on Economic Security report sent to Congress without health insurance recommendations(spelling out principles and promising further efforts to evolve a plan) • February- AMA House of Delegates passed a resolution declaring "unyielding opposition“ to Government health insurance • June- Health report of Committee on Economic Security, "Risks to Economic Security Arising Out of Illness," filed but not published, at the request of Roosevelt • July- First Government health insurance bill, the "Epstein bill" introduced in Congress • August- Social Security act passed- Congress authorized Social Security Board (Administration) to make “recommendations as to the most effective methods of providing economic security through social insurance and as to legislation and matters of administrative policy concerning old age pensions, unemployment compensation and related subjects."
The Fight Continues • 1938: The National Health Conference created the National Health Program that suggested legislative changes including: • Grants to the States for direct medical care programs those on public assistance rolls and those who were "medically indigent" (ordinarily self-sufficient but unable to meet the additional burden of paying for medical ) • Grants to the States to encourage the establishment of statewide health insurance programs financed either through general revenues or through social insurance taxes • Federal initiative to provide cash payments for disability due to illness. (It was suggested that temporary disability be established in a manner similar to unemployment insurance and that permanent disability be provided through the old-age insurance system.)
The Fight Continues • 1939: • February- Senator Robert F. Wagner introduces "National Health Bill" which incorporated the National Health program • AMA establishes "National Physicians' Commit-tee for the Extension of Medical Service" to fight Wagner bill. • April –July: Hearings on Wagner bill; proposal dies in committee. • September: WWII began and President Roosevelt turned his attention away from “purely domestic” matters • 1940: Roosevelt only included “hospital construction in his health affairs legislation, dropping the rest of the National Health Program
War-Time 1943-1950
War-Time Progress • 1942: • Representative Thomas Eliot introduces a precursor of National Health Insurance • Congress authorizes the Emergency Maternal and Infancy Care (EMIC)- a system of emergency health services for the dependents of servicemen, this was though to be a precedent for the passage of a health insurance system post-war • 1943: Original Wagner-Murray-Dingell bill introduced- provided for comprehensive health insurance under social security introduced. Congress takes no action on proposal.
Presidential Support • 1944: • President Roosevelt outlines in his state of the Union message an "economic bill of rights," including "the right to adequate medical care and the opportunity to achieve and enjoy good health“ and "the right to adequate protection from the economic fears of old age, sickness, accident, and unemployment." • The Social Security Board, in its eighth annual report to Congress, specifically calls for compulsory National Health Insurance as part of the social security system • April 1945: President Roosevelt dies
The Fair Deal • 1945: President Harry S. Truman , an enthusiastic supporter of the Health Bill proposal, sent a revision of the Wagner-Murray-Dingell bill to congress as apart of what he called “The Fair Deal” program • A heated debate ensued in the 5 years to follow and resulted in yet another defeat for the proponents of Government Health Insurance
Much of the groundwork that went into what would later become Medicare, was completed in the last 3 years of the Truman administration • 1950: • National Conference on Aging is convened by Federal Security Agency, which led to the Social Security Act amendments of 1950 which included grants to States for "vendor payments" in behalf of welfare recipients. • 1951: Social Security Administration annual report (1951) recommends health insurance for beneficiaries. • 1952: • Federal Security Administrator Oscar Ewing publicly proposes enactment of health insurance for social security beneficiaries. • Senators Murray and Humphrey, and Representatives Dingell and Celler, introduce bills embodying the beneficiaries idea- No congressional action taken. • President's Commission on the Health Needs of the Nation endorses such a program.
"I have had some bitter disappointments as President, but the one that has troubled me most, in a personal way, has been the failure to defeat the organized opposition to a National compulsory health insurance program. But this opposition has only delayed and cannot stop the adoption of an indispensable Federal health insurance plan.“ ~Harry S. Truman
The Home Stretch 1957-1965
Revival • 1956 was a year a revival of the debate over health insurance under social security • Four important events in congress occurred: • The enactment of the so-called military "medicare" program, a permanent program of Government health protection for dependents of servicemen • An expansion of payments to medical vendors for the provision of health care to welfare clients • Approval of a $30,000 study of the problems of the aged, out of which evolved a new Senate subcommittee charged with investigating this subject in depth • Adding to the social security program cash benefits for totally and permanently disabled persons aged 50 and over • 1957: Representative Aime J. Forand introduced a revised version of the beneficiaries-only health insurance proposal. This signaled the beginning of the fourth wave of the health insurance debate
Revival • December 1957: AMA House of Delegates resolves to defeat bill • Over the next 3 years this bill was hotly debated an re-introduced several times until it was finally defeated in 1960 • Also in 1960, The Ways and Means Committee reports Social Security amendments , including a new program of Federal grants to the States for medical services to the "medically indigent" elderly
The Home Stretch • 1964: • President Johnson sends special message, "Health of the Nation," to Congress, advocating Medicare • Medicare measure passes Senate (49-44) as a floor amendment to Social Security amendments (H.R. 11865) • July 30, 1965: Medicare (as part of the Social Security Amendments of 1965) signed into law by President Johnson.
The Medicare Plan (ca. 1965-66) • Private insurance companies selected to perform the major administrative functions of bill processing and benefit payment for Part A and Part B • All persons over 65 were automatically covered under Part A (hospital insurance), and Part B (supplemental medical insurance) was available for voluntary sign-up • Medicare Part A deductible: $40/yr • Medicare Part B premium: $3/ month • Total Medicaid Enrollment: 20 million by 1969
The Medicare Plan (ca.1970-1974) • Medicare Part A deductible: $52/yr • Medicare Part B premium: $4/month • Enrollment: 20.4 million • 1972: The Social Security Amendments of 1972 (signed by President Nixon) - Medicare eligibility extended to person under age 65 with long-term disabilities including ESRD and that had received SSID payments for 2 years • Developed professional standards review organizations and encouraged the use of Health Maintenance Organizations (HMO’s) • Medicare coverage expanded to chiropractic services, speech therapy, and physical therapy
The Medicare Plan (ca. 1975-1984) • Medicare Part A deductible: $92-$180/yr • Medicare Part B Premium: $6.70-$8.70/mth • Enrollment: 24.9-28.4 million • Health Care Financing Administration (HCFA) created to administer both Medicare and Medicaid Programs • Omnibus Reconciliation Act (OBRA) of 1980 • Expanded home health services by eliminating the limit on the number of home health visits, the prior hospital requirement and the deductible for any Part B benefits • List of outpatient surgical procedures that could be reimbursed on a prospective payment system ceveloped • “Baccus Amendments” or “Medigap” created supplemental insurance
The Medicare Plan (ca. 1975-1984) • The Tax Equity and Fiscal Responsibility Act (TEFRA) of 1982 • Increased Part B premium to cover 25% of program costs • Hospice Services added to covered benefits • Imposed a ceiling on the amount that Medicare would pay for hospital discharges • Required federal employees to begin paying HI payroll tax • Social Security Amendments of 1983 • Established an inpatient prospective payment system (PPS) which created pre-determined payments for treating diagnosis-related groups (DRGs)- replaced cost-based payment systems
The Medicare Plan (ca. 1975-1984) • The Deficit Reduction Act of 1984 • Froze physician fees and created the Participating Physician’s Program • Established fee schedules for laboratory services • Attempted to slow the growth of Medicare spending and constrain the federal deficit
The Medicare Plan (ca. 1985-1989) • Medicare Part A deductible: $400/yr • Medicare Part B premium: $15.50/month • Enrollment: 31.1 million • The Consolidated Omnibus Budget Reconciliation Act (COBRA) of 1985- Made Medicare coverage mandatory for newly hired state and local government employees • OBRA 1987- imposed quality standards on Medicare- and Medicaid- certified nursing homes
The Medicare Plan (ca. 1985-1989) • The Medicare Catastrophic Coverage Act of 1988 • Outpatient prescription drug benefits and a cap on out-of-pocket expenses • Expanded hospital and SNF benefits • Medicaid began coverage of Medicare premiums for beneficiaries with income below 100% of the federal poverty level (AKA Qualified Medicare Beneficiaries) • The Medicare Catastrophic Coverage Repeal Act of 1989- retracted major provisions of 1988 act included outpatient prescription benefits and out-of-pocket limit
The Medicare Plan (ca. 1990-1999) • Medicare Part A deductible: $592-$716/year • Medicare Part B premium: $28.60-$46.10/month • Enrollment: 34.3- 37.6 million • OBRA 1990- req’dState Medicare programs to cover premiums for beneficiaries with incomes between 100%-120% of the federal poverty level, expanded coverage to mammograms • The Health Insurance Portability and Accountability Act of 1996- established Medicare Integrity Program • Balanced Budget Act of 1997- Est. Medicare+Choice program ( a new structure for HMO’s), developed five new PPS’s
The Medicare Plan (ca. 2000-2009) • HCFA renamed Centers for Medicare and Medicaid Services • ALS coverage begins • Medicare Prescription Drug Improvement and Modernization Act (MMA) passed in 2003- provided new outpatient prescription drug benefits under Medicare beginning 2006 • First open enrollment for new Part D drug benefit • By 2008: • Part A deductible: $1024/year • Part B premium: $96.40/month • Avg. Part D premium: $27.93/month • Medicare Advantage Enrollment: 9.4 million • Part D Enrollment: 25.4 million • Total Enrollment: 44.8 million • Total Medicare Spending: $444 billion
Medicare Today and Tomorrow • Part B Premium $99.90/month • Total Enrollment: 49.4 million • Medicare Advantage Plan Enrollment: 11.5 million • The Medicare fund faces depletion sooner than the combined Social Security Trust Funds due to cost rising higher than GDP growth • Population aging - large baby-boom generation entering retirement and lower-birth-rate generations entering employment • Population aging caused by increasing longevity and health care cost growth somewhat more rapid than GDP growth.
“Lawmakers should not delay addressing the long-run financial challenges facing Social Security and Medicare. If they take action sooner rather than later, more options and more time will be available to phase in changes so that the public has adequate time to prepare. Earlier action will also help elected officials minimize adverse impacts on vulnerable populations, including lower-income workers and people already dependent on program benefits.” ~Social Security and Medicare Boards of Trustees in the SUMMARY OF THE 2012 ANNUAL REPORTS
References • Corning Peter A. THE EVOLUTION OF MEDICARE . . . from idea to law. 1969. http://www.ssa.gov/history/cornignappa.html. Accessed 9/29/2012 • “Medicare: A Timeline of Key Developments” The Henry J. Kaiser Foundation, 2012. http://www.kff.org/medicare/medicaretimeline.cfm. Accessed 09/29/2012 • Social Security and Medicare Boards of Trustees. SUMMARY OF THE 2012 ANNUAL REPORTS. http://www.ssa.gov/oact/trsum/index.html. Accessed 10/02/2012