Download
1 / 38
420 likes | 615 Views
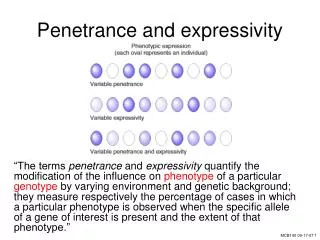
Penetrance Some manifestation or no expression % of people with the mutation that express the phenotype 50% penetrance = 50% of people with the gene show signs of it Expressivity Multiple or variable manifestations possible Different expressions of single gene

E N D
Penetrance • Some manifestation or no expression • % of people with the mutation that express the phenotype • 50% penetrance = 50% of people with the gene show signs of it • Expressivity • Multiple or variable manifestations possible • Different expressions of single gene • other genes or environmental factors may cause this modulation
MENDELIAN GENETICS • Anticipation • appearance of a trait to appear either earlier or more severe in subsequent generations • Fragile X • Myotonic dystrophy • Huntington Chorea
Genetics 101 Complex traits: • Polygenic: multiple genetic factors contributing to the phenotype, not one gene. • Add the environment • Modifier genes: Identified genes that influence the expression of a basic gene
gene 3 environment environment gene 1 gene 2 environment Genetics 101 “Complex” diseases have a genetic and environmental component Examples: • Asthma • Diabetes • Hypertension • Coronary Artery Disease • Alzheimer Disease • Schizophrenia • Depression Physical trait (disease)
Chromosomal Abnormalities Anaphase lag This leads to mosaicism: two different cell line Non-disjunction in a mitotic cell divisions can also lead to mosaicism
X-Inactivation and Disease in Females • Whether females are affected depends on • Degree of x-inactivation and in which tissues • Nature of gene product • The more the normal X is inactivated, the more symptoms the carrier female will show • Finding out more and more carrier females are indeed affected to varying degrees
X-inactivation • All X chromosomes except one are inactivated • Which X is inactivated is random • That X remains inactive for the life of the cell • Same X chromosome is inactive in all daughter cells
Imprinting • Some functional differences between the maternal and paternal chromosomes • Some genes need to be on or off during specific times during development • Genes are turned off by DNA methylation • Imprinted genes are “reset” in the gametes to reflect the sex of that individual
Chromosome Abnormalities • Translocations • Exchange of DNA between two (or more) chromosomes • Balanced if no material lost • 10% chance that there will be associated mental retardation of anomalies when de novo • Abnormal gametes • 25% normal • 25% balance like parent • 50% unbalanced
Chromosome Abnormalities • Robertsonian Translocation • Translocation between two acrocentric chromosomes • 13, 14, 15, 21, & 22 • Two long arms are combined into one chromosome • Short arms are lost • Encodes rRNA • Carriers are clinically normal • Prone to have reproductive problems
Genetic Screening • Current newborn screening • PKU, galactosemia • Hypothyroidism • Hemoglobinopathies (sickle cell disease) • Congenital deafness • Amino acid disorders • Organic acid disorders • Fatty acid oxidation disorders • Congenital adrenal hyperplasia • Cystic fibrosis • http://newborns.stanford.edu/Disorders.html#top
Genetic Screening • First trimester • Maternal Age • Nuchal translucency • PAPP-A • hCG • Second Trimester • Maternal Age • AFP • hCG • Estriol • Inhibin • Screen positive rate set at 5% • Current cut off is 1 in 150 on California X-AFP program • If screen negative, does not mean the fetus does not have the condition
Teratogens • Radiation exposure • Alcohol • Cocaine • Tobacco • Hyperthermia • Infectious agents • Maternal Diabetes • Maternal PKU • Drugs • Thalidomide • Methotrexate • Anticonvulsants (valproic acid, tegretol, dilantin) • Retinoic Acid
Karyotype • Usually from leukocytes or fibroblasts • Most karyotypes now are G banding • Gives light and dark bands • Identifies chromosomes • Photograph of chromosomes then “cut out” and paired • Look at chromosome numbers and gross structures
Routine vs. High Resolution • Routine karyotype is ~300-400 bands • Cell cycle stopped at metaphase • High resolution karyotype is 500+ bands • Cell cycle stopped earlier at prophase or prometaphase • More difficult to get significant cell populations stopped in earlier phases • More bands, more details to look for chromosomal structural abnormalities
Fluorescence In Situ Hybridization(FISH) • Used to look for missing or added chromosomal material not seen on karyotype • Need to use specific probes for the disease or condition • Also used to confirm findings on karyotype
Chromosome PaintingSKY • “Paints” entire chromosome with fluorescent color • Different colors for each chromosome • Used in cancer genetics • Usually multiple translocations and copy number abnormalities • Also used to identify “marker chromosomes” and other unknowns on karyotypes
Chromosomal Microarray • Able to look for copy number abnormalities in chromosomes • Cannot detect rearrangements where there is no change in copy number • Ability to detect deletions or duplications depends on density of probes
Polymerase Chain Reaction(PCR) • Used to amplify a specific region of DNA • Especially helpful in amplifying very small amounts of DNA • Eg. Forensics, Paternity testing • Diagnosis of single gene disorders where the mutations are well known such as cystic fibrosis, Sotos syndrome, Neurofibromatosis, Tuberosclerosis etc.
DNA Sequencing • Looking at sequence of DNA of a specific gene for mutations • Point mutations • Small deletions • Insertions • Cannot detect large deletions
Southern Blot Analysis • DNA moves through agarose gel at different speeds based on size • Smaller fragments move faster • Most often used after restriction enzyme digestion • Certain mutations cause loss or gain of restriction sites • “Blotting” is the transfer of DNA to nitrocellulose paper • Can then be treated with probes to make certain bands visible • Methylated DNA will move slower than unmethylated: expansion mutation testing
Pathogenetic Mechanisms • Deformation • Aberrant mechanical forces that distort otherwise normal structures • Disruption • Actual destruction of previously normal tissue • Dysplasia • Abnormal cellular organization of function within a specific tissue type • Malformation • Failure or inadequate completion of one or more of the embryonic processes with early development of a particular tissue or organ system being arrested, delayed or misdirected
Clinical Classifications of Birth Defects • Single System Defects • Malformations that involve only a local region of a single organ system • Cleft lip, club foot, congenital hip dislocation, congenital heart disease • Associations • Physical features that are associated in a nonrandom fashion but the link is not strong or consistent enough to justify a definition of a syndrome • VATER/VACTERL Associations • Sequences • Pattern of multiple malformations that can be shown to be the result of a cascade of consequences from a primary defect • Potter sequence, Pierre-Robin sequence • Complexes • Existence of a noxious influence that acts on a particular geographic part of the developing embryo that results in abnormalities of adjacent structures • Vascular anomalies • Syndromes • Congenital abnormalities that occur in combinations that are more or less fixed giving a consistent pattern (syndrome is from the Greek “running together”) • Down Syndrome, Hunter Syndrome, Fragile X Syndrome
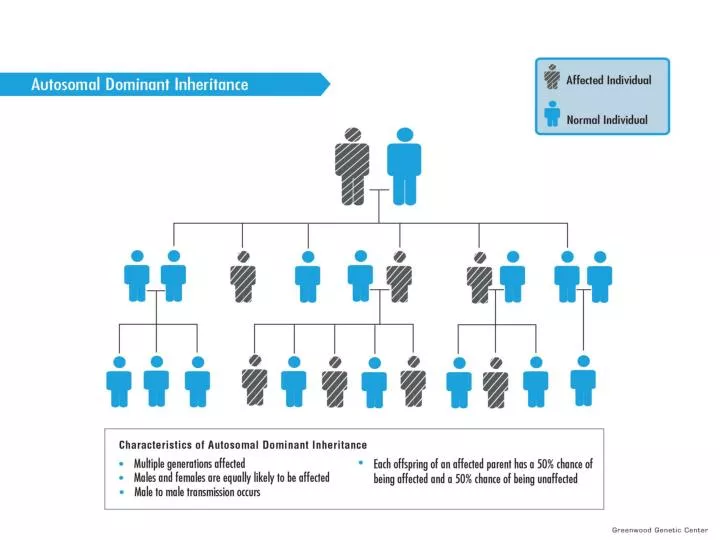
Breast Cancer • 1. What factors suggest that Rachel is at risk for hereditary breast cancer? • Cancer in first degree relatives • Early age of onset of disease in first degree relatives • Bilateral breast cancer in III-2 • Ovarian cancer in III-1 & III-9 • 2. What is the likely mode of inheritance? • Autosomal dominant trait is suggested by inspection of family tree. • The features of disease in this family suggest BRCA1 which is known to be inherited as an autosomal dominant.
Breast Cancer • 3. What mechanism(s) do you think might explain the high risk of cancer in some families? • Both genetic and environmental factors could be important. • Love Canal would be an example of environmental situation (toxic waste) that might lead to multiple members of a family having disease. • Genetic syndromes include those with mutations in tumor suppressor genes, oncogenes and DNA repair genes.
Huntington Disease • 2.What is the chance that Joe might develop Huntington disease? • mean onset of HD is 35-44 years. • Autosomal Dominant (with Delayed Age of Onset). • Chance of Bob’s father having the HD gene: 50%, and Thomas is his brother, 50% chance to share the same gene => 50% x 50% = 25% => the chances of Joe having this gene 50% x 25% = 12.5%. • If Bob’s parents did not have HD manifestations at an old age we might suspect that there was a recent expansion of an intermediate allele (27 to 35 repeats) that can occur in ~ 2.5% of alleles transmitted by the father accounting for Bob’s disease. • Possibility of paternity issues must also be considered since new mutations are extraordinarily rare.
Triplets and Huntington • There is a strong inverse correlation between • the number of repeats and age of onset of Huntington’s disease.
Down syndrome, trisomy 21 • 1. What type of chromosomal abnormality that can cause Down syndrome does the couple not know? Which partner do you want to test and why? • The father since the Down syndrome child born to a 29 year old mother may have a translocation inherited from his parents. • Down’s patients born to mother under age 30 • 10% due to unbalanced translocation • 50% de novo mutations • 50% inherited • First degree relative have 50% chance carrying the translocation • The father’s chance of having the translocation 10% x 50% x 50% = 2.5%
Down Syndrome • Down syndrome is a congenital condition causing mental retardation and unique physical characteristics. • Some characteristics may be flattened face and occiput, upwardly slanted eyes, a large tongue, small low set ears, short stature, small nose with low nasal bridge, an extra skin fold at the medial aspect of the eyes (epicanthal folds) • These individuals have an extra chromosome 21 and may have congenital heart problems, gastrointestinal anomolies, and hearing loss. www.down-syndrom.ch/ ds_netring.htm
Turner Syndrome 1. Justify the expense of a karyotype to Theresa's insurance company.(Hint: you might want to review some of the clinical features of Turner syndrome.) Clinical features include: 1. short stature 2. minor anomalies of face and extremities 3. lymphedema (hands/feet at birth; webbed neck) 4. congenital heart disease (20%) - coarctation of aorta 5. renal abnormalities (50%) 6. gonadal dysgenesis (streak ovaries) - lack of secondary sex characteristics; amenorrhea; infertility • Theresa has Turner syndrome there is a risk that she might have mosaicism. • ~5% of Turner patients have some XY cell lines. These individuals have a 20% risk of malignancy of the dysgenic gonad. www.weblo.com
Fetal Alcohol Syndrome • Growth deficiency • Smooth philtrum • Thin vermilion • Small palbebral fissures • Brain damage • Developmental delays • Ventricular septal defect