Download

1 / 44
440 likes | 565 Views
IMMUNISATIONS. Immunisations. The immunisation programme in the UK evolves Population immunity if high enough enables the unimmunised to be protected Vaccination enabled smallpox to be eradicated in 1980 WHO is working towards global polio eradication. Acquired immunity.

E N D
Immunisations • The immunisation programme in the UK evolves • Population immunity if high enough enables the unimmunised to be protected • Vaccination enabled smallpox to be eradicated in 1980 • WHO is working towards global polio eradication
Acquired immunity • Is specific to a single or a group of closely related organisms • Active immunity can be acquired by natural disease or immunisation • Is either antibody or cell mediated
Passive Immunity • Is the transfer of active humeral immunity in the form of ready made antibody • Passive transfer occurs when antibody passes from mother to child • Artificially acquired transfer occurs when antibody or antitoxin from an immune individual (or animal) is given to an individual at risk • Useful when • there is a high risk of infection • there is insufficient time for the body to produce its own response • where the individual is immunodeficient
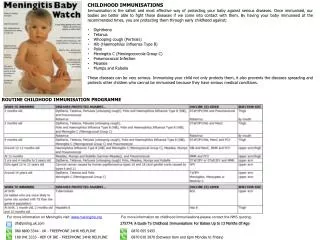
MEASLES • Viral, droplet spread, incubation 10 days • Coryza, conjunctivitis, fever, rash • Complications: pneumonia,encephalitis,death • Notifiable • Catch up programme offered to those with incomplete immunisation because of increasing notifications
MUMPS • Viral,droplet spread, incubation 14-21 days • Parotid swelling • Complications: oophritis, orchitis, pancreatitis, and meningitis • Notifiable
RUBELLA • Viral, droplet spread incubation 14-21 days • Mild illness with rash and lymphadenopathy • Maternal rubella, 1st trimester 90% foetal damage ( microcephaly, deafness, cataracts, PDA etc) • History needs confirmation with saliva or serology
Chicken pox vaccine • Given routinely elsewhere, not in UK • Cost? • Possible increase in Herpes Zoster if immunity is not gained by natural infection?? • Available for children at risk
Note:-- Zoster vaccine available to the over 70-79s September 2013
DIPHTHERIA • Corynebacteria diphtheriae • Incubation 2-5 days Infectious for four weeks • Inflammatory exudate causing grey membrane in resp tract. Potential obstruction • Toxin mediated damage to myocardium, nervous system and adrenals
TETANUS • Toxin mediated from tetanus bacillus • Incubation 4-21 days • Spore spread • Muscular rigidity with spasms ---(lock jaw)
POLIO • Polio virus • Faecal/oral spread, Incubation 3-21 days • Virus may be shed for 6 weeks • Range of severity--- asymptomatic to paralysis
PERTUSSIS • Bordetella pertussis • Incubation 7-10 days • Infectious until 3 weeks after onset of paroxysms • Paroxysmal cough can be associated with apnoea and /or vomiting • ‘The 6 month cough’ • Complications--- SUDI, bronchopneumonia and cerebral hypoxia
HAEMOPHILUS INFLUENZAEType B • Hib • Meningitis with high incidence of complications +/- bacteraemia • Epiglottitis • Osteomyelitis
MENINGOCOCCAL DISEASE • Neisseria meningitidis • Type C vaccine, Type B vaccine being developed— • (also available Type A for travelers) • Incubation 2-3 days • Onset can be fulminant • Meningitis / septicaemia • Fever, vomiting, purpuric rash
Routine Immunisation schedule • 2 months Diphtheria Pertussis Tetanus Hib Polio and Pneumococcal (PCV) +Rotavirus • 3 months Diphtheria Pertussis Tetanus Hib Polio and Men C + Rotavirus • 4 months Diphtheria Pertussis Tetanus Hib Polio and Pneumococcal and Men C
Routine Immunisation schedule • 12-13 months Men C and Hib MMR and Pneumococcal • 2-3 yrs Influenza • 3 to 5 yrs Diphtheria Pertussis Tetanus Polio and MMR • 12-13yrs Human papilloma virus vaccine 3 doses ( girls only) • 14 yrs Diphtheria Tetanus Polio Check MMR status
Active Immunity • Live Attenuated Vaccines eg BCG, MMR, yellow fever, oral polio, oral Rotavirus, nasal influenza (from September 2013) • Inactivated Vaccines eg influenza • Extracts of or Detoxified Endotoxins eg tetanus
Passive Immunity • Normal Immunoglobulin eg for replacement therapy of agammaglobulinaemia • Specific Immunoglobulin eg tetanus, VZV, rabies, HepB and palivizumab for RSV protection
Contraindications To Vaccination • General – Febrile illness • Anaphylaxis to previous dose or to components of vaccine • Severe local reaction • Inconsolable unexplained crying >3 hrs within 72hrs • Encephalopathic illness (hypotonic-hyporesponsive episode (HHE) within 72 hours • Intramuscular route should not be used for children with bleeding disorders—use s.c. route • Live Vaccines – Immunosuppressed, e.g. prednisolone therapy, chemotherapy, HIV (note MMR can be if not severely imunocompromised), BMT within 6 months. Pregnancy
DTaP/IPV/Hib and MenC • Diptheria, Tetanus, acellular pertussis, Inactivated polio , Haemophilus influenzae and Meningitis C • Recent changes are inactivated polio (im) and acellular pertussis • Well tolerated, minimal side effects • For children over 10 years adsorbed diphtheria (low dose),Tetanus and inactivated polio vaccine only if have received primary immunisations
MMR • Measles, Mumps and Rubella • Serious illnesses associated with significant mortality • Fever common 6 to 10 days post vaccination • 1:1000 febrile convulsion • Can be given to egg allergic children • NOT associated with Autism and IBD
Current measles prevelence • First 6 months 2011------497 cases in UK • First 6 months 2012------964 • Significant increase in South Wales 2013 • Most in the 10-12 age group
BCG • Administered to at risk babies in neonatal period ( where incidence is greater than 40 per 100,000) • Given intradermally • Since 2006 risk-based programme for other children as well • Local Side effects common--- ulceration or abscess • Do not give to HIV + or immunocompromised Mantoux induration > 6mm Previous BCG or past/ present TB.
PNEUMOCOCCAL VACCINES • Prevenar < 2yrs • Since 2010 13-valent available • Part of the routine schedule. • Pneumovax > 2years 23- valent polysaccharide • Indications for Pneumovax • not previously immunised, asplenia, SS disease, chronic lung or heart disease
Rotavirus Vaccine • Rotavirus is responsible for 1 in 10 hospital admissions in children • Immunisation in UK introduced September 2012, routine from July 2013 • Live attenuated oral vaccine • Two doses four weeks apart • Effective after 6 weeks of age • To be offered at 2 and 3 months in the vaccination Schedule
Influenza vaccine • Trivalent inactivated influenza vaccine(TIV) licenced from 6 months • Live attenuated influenza vaccine available • nasal spray (LAIV), licenced in Europe for 2-17s • LAIV contains 3 strains. • Not licenced for <2s • 2 doses one month apart, unless previously immunised when one is sufficient. • Piloted 2013, roll out to <5s this year and all children 2015
OTHERS • RSV - passive immunisation—Palivizumab-(Synargis) –given during RSV season to high risk groups. Monoclonal antibody given monthly. • HepBV – at risk groups (at present) • HPV – Human Papilloma Virus vaccine -3 doses Given to 12-13 year olds –due to increase coverage to 17-18 year olds in September 2008 Cervarix—effective against Type 16 &18 HPV Protects against 75% of cervical cancers Gardasil introduced Sept 2012—effective against Type 6,11, 16 &18 –hence against 90% genital warts as well
Others (cont) • Chicken pox routine in USA at 12-15 months/top up at 5/6years. Available but not routine in UK. • Meningococcal B vaccine available from January 2013, but not in immunisation schedule yet. • Pertussis vaccine now advised for every pregnant woman between 28 and 38 weeks ( new recommendation)
Vaccine ANAPHYLAXIS ABC Adrenaline 10 mcg/kg (0.01ml/Kg 1:1000) Hydrocortisone 4mg/kg Chlorphenamine Beware neomycin and gelatin anaphylaxis – omit MMR