Download
1 / 25
290 likes | 973 Views
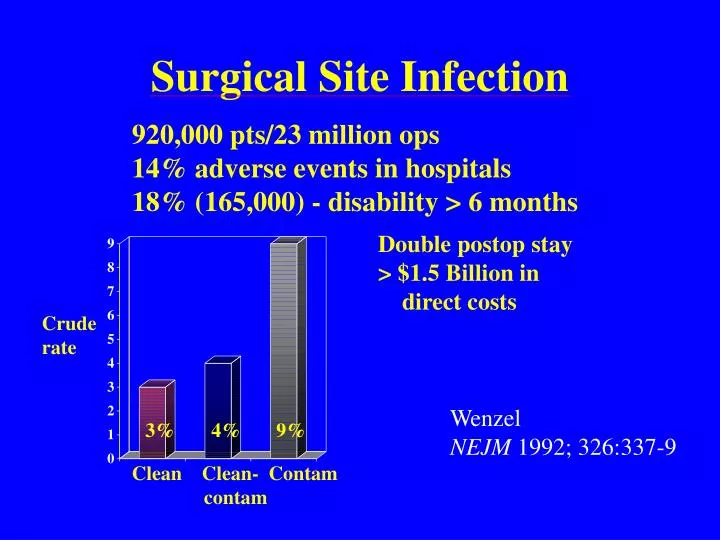
Surgical Site Infection. 920,000 pts/23 million ops 14% adverse events in hospitals 18% (165,000) - disability > 6 months. Double postop stay > $1.5 Billion in direct costs. Crude rate. Wenzel NEJM 1992; 326:337-9. 3%. 4% 9%. Clean Clean- Contam contam.

E N D
Surgical Site Infection 920,000 pts/23 million ops 14% adverse events in hospitals 18% (165,000) - disability > 6 months Double postop stay > $1.5 Billion in direct costs Crude rate Wenzel NEJM 1992; 326:337-9 3% 4% 9% Clean Clean- Contam contam
Surgical Site Infections in Presence or Absence of a Remote Infection 32% no yes 25% 18% 15% rate 10% 7% 6% Ann surg 1964; 160
Relationship Between Wound Infection Reporting and Subsequent Infection Rates N=(1500) (1447) (1743) (1939) Cruse Canad Med Assoc J 1970; 102: 251 % Pre Post Pre Post Hospital A Hospital B
Influence of Shaving on POW Infection Rates Rate (%) 9 10 8 3.5 - razor - - clipper - Alexander et al Arch Sgy 1983
Timing of Prophylactic Antibiotics and Risk of Surgical Wound Infection Prospective cohort 2847 patients clean/clean-contaminated sgy Timing SWI Early prep (364) - 3.8% Preop (1709) - 0.6% Periop (282) - 1.4% Postop (488) - 3.3% Classen et al NEJM 1992; 326:281-6
Mupirocin study to prevent S. aureus POW infections - University of Iowa Prospective, randomized, double-blind placebo-controlled N=3966 patients at U of Iowa Preop carriage of S. aureus 891 (22%) Perl et al IDSA 1999
Mupirocin vs Placebo in Preoperative Patients Mupirocin Placebo (n=1933) (n=1933) Noso inf 218 (11%) 220 (11%) SSI 152 (8%) 164 (9%) S. aureus Nosoinf 45 (2.3%) 55(2.99%) S. aureus SSI 43 (2.2%) 46 (2.49%) Perl et al
The MARS Study: 2% Mupirocin Preoperatively to Prevent S. aureus Infections 4030 patients (23% nasal carriers) Elim nasal carriage 80% 3 doses 93% 6 doses 18% TCV 18% nsgy 64% gen sry % elim carriage 8.3% 80.2% Perl, Cullen, Wenzel et al
The MARS Study: 2% Mupirocin Preoperatively to Prevent S. aureus Infections ALL PATIENTS CARRIERS S. a inf S a SSI p=0.02 percent 7.9 2.3 8.5 2.9 9.9 3.8* 11.6 7.6* Perl, Cullen, Wenzel et al
Surgical Technique: SSIs and Midline Incisional Hernias Mean SSI 10%(0-27%) SL:WL ratio mean hernia 15% (5-26%) <4 - 22% hernia 1013 patients >4 - 9% hernia SSI predictors Hernia predictors OROR age(y) .986 age (y) 1.022 obesity 2.02 obesity 2.45 optime(h) 1.003 wound inf 2.5 deg.contam 1.85 sliwl<4 2.98 reop 3.32 Israelsson Eur J Surg 1998;164:353
Perioperative Normothermia and the Incidence of Surgical Wound Infection Hypothesis: Hypothermia with vasoconstruction pO2 , phagocytosis, and infection Plan: Randomized, double blind, controlled study of colorectal sgy pts Intervention: IV fluid warmers and forced warm air to up. body Standard: Bowel prep, preop ab Mean temp: 34.7 º C vs 36.6 º C Kurz et al NEJM 1996; 334:1209-15
Perioperative Normothermia and the Incidence of Surgical Wound Infection and Hospital Stay Colorectal surgery patients p=0.009 p=0.01 13.5 19 11.8 6 LOS (d) Inf. rate (%) Kurz et al NEJM 1996; 334:1209-15
Supplemental Perioperative Oxygen and Rate of Surgical Wound Infection Hypothesis: oxidative killing is most imp defense vs POW infection Plan: randomize 500 pts undergoing colorectal sgy electively Intervention: 30% vs 80% inspired 02 via mask up + 2 h post op Standard: bowel prep, anesthesia, antibiotics core temp 36º C Pulse Ox: 97% vs 99% (p<0.001) Subcu Ox tension mmtg: 54 vs 73 (p=0.02)
Supplemental Perioperative Oxygen and Rate of Surgical Wounds Infection Mortality: 2.4% (30%) vs 0.4% (80%) p=0.13 11.2 Inf rate (%) 5.2 oxygen Greif et al NEJM 2000; 342:161-7
Life Threatening Pelvic Sepsis After Stapled Hemorrhoidectomy 24 48 72 post-op hour Lancet 2000; 355: 810
28 year old woman with post-op fever after liposuction • Disorientation • septic shock • buttock, thigh grey • inter necrosis • death • Buttocks and • thigh liposuction • f, ch, myalgia • N, V, D • op site pain, • tender, minor erythrema • swelling • broad-spectrum • antibiotics • Necrotic areas excised • open incision • drains • ARDS • dialysis • hypotension 0 1 2 3 4 5 P o s t-op d a y Anesth Plast Surg 2000; 24: 344-7
Necrotizing Fasciitis Rare, rapidly progressing 30-60% mortality 38% (delay) vs 4% immed surgery S. pyogenes or anerobes/GNR Grey, edematous sq fat strips off fiscia c finger Aesth Plastic Surg 2000; 24: 344-7 Ann Surg 1998; 64:397
Barriers to Effective Treatment of Necrotizing Soft Tissue Infections Delays in diagnosis Inadequate debridement Phys exam Work up Surgery • not “simple cellulitis”! • more pronounced pain, toxicity • no undue delays with CT, MRI • surg exploration more efficient with frozen section • not ITS! But • repeated, excisional debridement Urschel Postgrad Med J 1999; 75:645-9
10 year old boy post op fever and rash • closed reduction depressed nasal fx 1x1 cm2 gelfoam support • ER: f, n, v, abd pain 120/min mac rash face tr , abd gelfoam removed: no pus • discharged well 0 1 2 3 4 5 6 post-op day
Early ( 48 hours) Post-operative Infectious Diseases Emergencies Toxic Shock Syndrome Streptococcus pyogenes Clostridium species Necrotizing fasciitis
Necrotizing Soft Tissue Infections Necrotizing fasciitis • Type I Polymicrobial Risk: DM Rx pen(vanc) gas in most anti-anerobe 3rd gen ceph • Type II gas ± S. aureus Risk: 50% gas TSS, varicella, NSAIDS, Pen +climdes rapid necrosis mult +/- IVIG tissue levels Gas gangrene • C. perifringens fulminant pen + clindes myonecrosis gas ? Hyperbaric O2 Urschel Postgrad Med J 1999; 75:645-9
Toxic Shock Syndrome 1978 - Described by Todd et al Lancet 1978; 2:1116-8 1980 - TSS + Tampon use NEJM 1980; 303:1429-42 Attack rate after nasal sgy 16,5/1000,000 + 10% mortality J Infect Dis 1986; 153:356-9 major (4) minor (3) fever, rash, BP GI/m-sk/liver desquamation heme/cns involv Otolaryn Head Neck Surg 1999; 120:569-70
Botryomycosis Rare, indolent infection Pseudomycosis, suppurative Underlying immunodeficiency and/or tissue with poor healing ability Histo: organisms (granules) surrounded by neutrophils in fibrocellular stroma
Streptococcal TSS (T1, M-1) in 2 Patients Infected by a Colonized Surgeon 2 d post op gen rash bluish skin wound 85/50 125 378 GAS - wound 73/39 105 386 erythema red, swollen arm Nasal carrier GAS 43 male Inguinal hernia repair 55 woman tetanus toxoid vaccine Rutishauser et al Infection 1999; 27:259
Preventing Post-op Wound Infections Pre-op advice Perioperatively Operativly Post-op • Colon sgy: • temp>36ºC • 80% O2 via • mask • stop smoking! • optimize nutrition • and weight • seek hi-volume • hospital/surgeon • with rates reporting • control comorbid • cure remote inf. • Avoid shaving • approp.antibiotics • and timing • consider mupirocin • in carriers • 80% O2 • f 2 h • D/c devices • appropriately