Download
1 / 47
610 likes | 1.22k Views
Radiation Skin Reactions. Peter R Hancock RN. Learning Outcomes . Recognise Levels/grades of radiation Skin reactions Gain Knowledge with regards to correct evidence based care for management of radiation skin reactions Recognise possible incorrect care procedures

E N D
Radiation Skin Reactions Peter R Hancock RN
Learning Outcomes • Recognise Levels/grades of radiation Skin reactions • Gain Knowledge with regards to correct evidence based care for management of radiation skin reactions • Recognise possible incorrect care procedures • Gain increased ability to adapt care procedures for individual patient scenarios
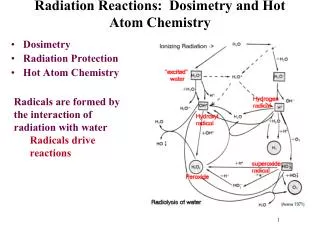
What are Radiation Skin Reactions • An outward manifestation of cellular effect of radiation therapy on the skin • As radiation travels through the skin to treat the disease process, it “interferes” with skin cells’ ability to regenerate, resulting in dry, red, itchy, and sometimes painful skin in the treatment area. • Radiation works by breaking/Damaging DNA molecules inside the cancer cell, which in turn keeps the cell from growing, dividing, and spreading
Measurement Scales • RTOG (Radiation Therapy Oncology Group) • RisRas (Radiation Induced Skin Reaction Assessment Scale)
RTOG • Includes a simple 0 – 4 scaling • 0 = no reaction • 1= faint erythema, dry desquamation, epilation • 2= moderate erythema, wet desquamation, oedema • 3= Widespread erythema, wet desquamation, intense oedema • 4= ulceration haemorrhage, necrosis
RTOG • Used for over 25 years • Is it the best system? • What are you thoughts?
Limitations • One limiting factor of the RTOG scale is that dry desquamation and erythema are scored equally on the scale, yet the appearance of either side effect can vary dramatically from patient to patient • Eg : A patient received radiation treatment for head and neck or oesophageal cancer can suffer severe dry desquamation, in which the affected skin can become cracked and painful
Limitations • The development of erythema presents quite differently yet the RTOG scale rates both reactions with the same score. • A further limitation of the scale is that the scale is quite subjective. The scale only measures reactions by the clinical judgement of the nurse in question and has no facility for patient feedback
Positive Points • It has been shown within this literature that skin assessments performed by clinical professionals using this scale have been able to pinpoint patients who are at risk of progressing to a higher RTOG scale rating, thus allowing for preventative interventions to be implemented • In the clinical enviroment it is shown that the ease of use of the RTOG scale allows for the most inexperienced clinician or reliever to effectively use the scale to plan their care interventions
Positive Points • Concurring literature proceeds to show evidence that experienced clinicians can use their experience to account for the shortfalls of the scale whilst providing evidence based wound care for the patients • My experience is that patient assessments in radiation outpatient units are conducted daily, the shortfalls described in the literature can be seen as inconsequential when this is the clinical practice.
Risras • Developed by Noble-Adams in 1999 • rectifies the RTOG issue of differences in treatment side effects • Includes both a patient self reporting symptom scale and a clinical professional variance scale
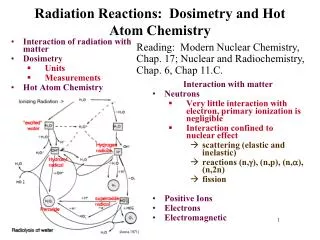
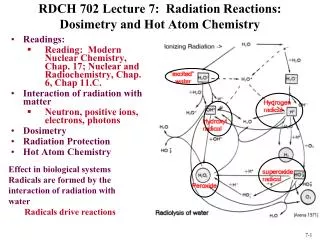
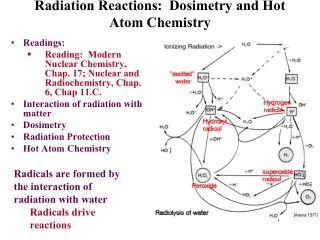
Conceptual Framework of predictors for radiation skin reactions
Caring for radiation skin reactions • Hygiene cares conducted with lukewarm water and mild-sensitive soap is now recommended as routine care for all patients receiving any form of radiation therapy • There is inconclusive evidence to recommend any particular sensitive soap to wash with whilst receiving radiation treatment. General data garnished from dermatology sources, anecdotal nursing reports all suggest that patients use ph-neutral or non alkalating soap during treatment
Caring for Radiation Skin Reactions • There is a study conducted by Frosch and Klingman (1979) that determines the irritant tendencies of soaps by using a soap chamber. This study showed that Dove sensitive soap made by unilever as the only technically “mild” soap out of eighteen tested varieties • As hygiene care and shampooing hair are socially expected norms preventing patients from adhering to their normal routines may cause additional emotional stressors without any proven benefits
Caring for Radiation Skin Reactions • The usage of deodorant in the specific area of treatment has created a large amount of clinical controversy as there are concerns that there may be an increase in surrounding surface skin doses caused by potential bolus effects of having matter on the skin surface • Due to the effect that radiation therapy has on the sweat glands the need for deodorising therapy is diminished significantly after the first few weeks of radiation therapy.
Caring for radiation skin reactions • A study conducted by Burch in 1997 used a specially designed ionization chamber to measure the surface dose of 15 deodorising products and there ingredients. Samples were compared between normal application thickness and a sample size 5 times thicker than normal • There was no reported increase in surface dose with normal application of deodorant. No difference was reported between metallic based and non-metallic based deodorising products
Caring for radiation skin reactions • This directly challenged the previous cannon that products containing magnesium, aluminium or zinc would increase surface dose leading to an increase in radiation skin toxicities • Some Studies suggest that an increase in radiation skin reactions may be attributed to irritating chemical ingredients in the products such as sodium laureth sulphate rather than a bolus effect with normal deodorant application.
Caring for radiation skin reactions • Due to the granulating nature of healing wounds knitted cellulose acetate dressings such as adaptic™ are used to prevent the wound bed from adhering to the external dressing • Hydrogel products are used to effect autolytic debridement and prepare the wound bed in all types of wounds
Radiation Skin Care • Intrasite Gel’s partially hydrated formulation allows the gel to donate moisture to drier environments and absorb in wetter environments, creating a moist wound healing environment. • moisturizing of the skin in the treatment area at least twice a day during the treatment. This moisturizing routine should continue for at least six months as per studies after the treatment. This in theory allows for the area to retain its elasticity and prevent radiation recall
References • Adams, L. (2009). Managing side effects in radiation therapy patients. Radiation Therapist, 18(2), 109-123. • Aistars, J. (2006). The validity of skin care protocols followed by women with breast cancer receiving external radiation. Clinical Journal of Oncology Nursing, 10(4), 487. • Aistars, J., & Vehlow, K. (2007). A pilot study to evaluate the validity of skin care protocols followed by women with breast cancer receiving external radiation. Oncology Nursing Forum, 34(1), 219-219. • Aquino-Parsons, C., Lomas, S., Smith, K., Hayes, J., Lew, S., Bates, A. T., et al. (2010). Phase III study of silver leaf nylon dressing vs standard care for reduction of inframammary moist desquamation in patients undergoing adjuvant whole breast radiation therapy. Journal of Medical Imaging & Radiation Sciences, 41(4), 215-221. • Bartholomay, M., Mannix, C., Barton-Burke, M., Bilodeau, M. L., Delaney, R., Doherty, C., et al. (2008). A feasibility study of low-cost patient-administered skin care intervention among head and neck cancer patients receiving chemo-radiation. Oncology Nursing Forum, 35(3), 494-494. • Bieck, P., & Phillips, S. (2009). Appraising the evidence related to avoidance of the use of lotions or topical agents prior to radiation therapy. Oncology Nursing Forum, 36(3), 45-45.
References • Bieck, T., & Phillips, S. (2010). Appraising the evidence for avoiding lotions or topical agents prior to radiation therapy. Clinical Journal of Oncology Nursing, 14(1), 103-105. • Bojen, A. (2007). Skin care after radiation therapy: evidence contra tradition [sic] [Danish]. Sygeplejersken / Danish Journal of Nursing, 107(12), 44-54. • Bolderston, A. (2003a). Skin care recommendations during radiotherapy: A survey of Canadian Practice. Canadian Journal of MRT, 34, 3-11. • Bolderston, A. (2003b). Skin care recommendations during radiotherapy: a survey of Canadian practice. Canadian Journal of Medical Radiation Technology, 34(1), 3-11. • Bolderston, A., Lloyd, N., & Wong, R. (2005). The prevention and managment of acute skin reactions related to radiation therapy: program in evidence based care. Cancer Care Ontario, 13(7) • Campbell, I. R., & Illingworth, M. H. (1992). Can patients wash during radiotherapy to the breast or chest wall? A randomized controlled trial. Clinical Oncology, 4(2), 78-82. • Campbell, M. K., & Pruitt, J. J. (1996). Radiation therapy. Protecting your patient's skin. RN, 59(1), 46-46. • Cibul, J., & Starita, A. (2001). Skin savvy: coping with a common side effect of radiation therapy. MAMM, 3(6), 46.
References • Cibul, J., & Starita, A. (2002). Companion Summer 2002: ideas and resources for recovery. Skin savvy: coping with a common side effect of radiation. MAMM, 2A(2), 32-33. from • Cox, C. E. (2006). Self-help. To protect and soothe: skin care during radiation therapy. MAMM, 8(1), 54-55. • Currie, G., & Wheat, J. (2006). Wheatgrass extract as a topical skin agent for acute radiation skin toxicity in breast radiation therapy. Journal of the Australian Traditional-Medicine Society, 12(1), 7-11. • D'Haese, S., Van Roy, M., & Bate, T. (2010). Management of skin reactions during radiotherapy in flanders: a study of nursing practice before and after the introduction of a skin care protocol. European Journal of Oncology Nursing, 14, 367-372. • D'Haese, S., Van Roy, M., Bate, T., Bijdekerke, P., & Vinh-Hung, V. (2010). Management of skin reactions during radiotherapy in Flanders (Belgium): A study of nursing practice before and after the introduction of a skin care protocol. European Journal of Oncology Nursing, 14(5), 367-372. • Davies, A. (2003). Wound care. Nursing a patient with a malodorous fungating non-healing wound. Nursing Times, 99(13), 58.
References • Davies, P., & Rippon, M. (2008). Evidence review: the clinical benefits of SAFETAC technology in wound care. Journal of Wound Care, 4-31. • Dest, V. (2000). Consult stat. Helping patients cope with skin problems caused by radiation. RN, 63(2), 73-73. • Devita, V., Lawrence, T., & Rosenberg, S. (2008). Cancer Principles & Practice of Oncology (8th ed.). Philadelphia, PA 19106 USA: Lippincott Williams & Wilkins. • Draper, C. (2005). The management of malodour and exudate in fungating wounds. British Journal of Nursing (BJN), 14(11), S4. • Dunne-Daly, C. F. (1995). Skin and wound care in radiation oncology. Cancer Nursing, 18(2), 144-160. • Erwin-Toth, P. (2007). Skin changes from radiation therapy. Journal of Wound, Ostomy & Continence Nursing, 34(5), 546-546. • Faithfull, S., Hilton, M., & Booth, K. (2002). Survey of information leaflets on advice for acute radiation skin reactions in UK radiotherapy centres: a rationale for a systematic review of the literature. European Journal of Oncology Nursing, 6(3), 176-178. • Fenton-Kerimian, M., & Cartwright, F. (2008). A pilot study of the optimal topical agent to minimize radiation dermatitis during whole breast irradiation given as part of breast conserving therapy. Oncology Nursing Forum, 35(3), 540-540.
References • Fitzgerald, T. J., Jodoin, M. B., Tillman, G., Aronowitz, J., Pieters, R., Balducci, S., et al. (2008). Radiation therapy toxicity to the skin. Dermatologic Clinics, 26(1), 161-172. • Frosch, P., & Klingman, A. (1979). The Soap Chamber: A new method of testing the irratancy of soaps. Journal of Academic Dermatology, 1, 35-41. • Giordano, S. (2010). Radiation-induced skin injuries during interventional radiography procedures. Journal of Radiology Nursing, 29(2), 37-47. • Gosselin, T. K., Schneider, S. M., Plambeck, M. A., & Rowe, K. (2010). A Prospective Randomized, Placebo-Controlled Skin Care Study in Women Diagnosed With Breast Cancer Undergoing Radiation Therapy. Oncology Nursing Forum, 37(5), 619-626. • Heggie, S., Bryant, G. P., Tripcony, L., Keller, J., Rose, P., Glendenning, M., et al. (2002). A phase III study on the efficacy of topical aloe vera gel on irradiated breast tissue. Cancer Nursing, 25(6), 442-451. • Hill, S. (2005). Notes on practice. Managing radiation skin injury. Ostomy Wound Management, 51(10), 26. • Hodge, H., Indra, J., Drobeck, H., Duprey, L., & Tainter, M. (1972). Acute Oral toxicity of methylrosaniline chloride. Journa of Toxicology and Applied Pharmacology, 22(1), 1-5.
References • Hogle, W. P. (2007). Radiation therapy in the treatment of breast cancer. Seminars in Oncology Nursing, 23(1), 20-28. • Hollinworth, H., & Mann, L. (2010). Managing acute skin reactions to radiotherapy treatment. Nursing Standard, 24(24), 53. • Hunter, S., Langemo, D., Thompson, P., Hanson, D., & Anderson, J. (2007). Research forum. Radiation wounds. Advances in Skin & Wound Care, 20(8), 438. • Jones, J. (1998). How to manage skin reactions to radiation therapy. Nursing, 1-2. • Korinko, A., & Yurick, A. (1997). Maintaining skin integrity during radiation therapy. American Journal of Nursing, 97(2), 40-44. • Kumar, S., Juresic, E., Barton, M., & Shafiq, J. (2010). Management of skin toxicity during radiation therapy: A review of the evidence. Journal of Medical Imaging and Radiation Oncology, 54(3), 264-279. • Lambertz, C. K., Gruell, J., Robenstein, V., Mueller-Funaiole, V., Cummings, K., Knapp, V. (2010). NO SToPS: reducing treatment breaks during chemoradiation for head and neck cancer. Clinical Journal of Oncology Nursing, 14(5), 585-593. • Laverty, D. (2010). Managing fungating wounds: a multifactorial approach. European Journal of Palliative Care, 17(1), 6-9.
References • Mak, S. (2000). The effects of hydrocolloid dressing and genitian violet on radiation induced moist desquamation wound healing. Journal of cancer nursing, 23, 220-229. • Margolin, S. (1990). Management of Radiation induced moist skin desquamation using hydrocolloid dressings. Journal of cancer nursing, 13, 71-80. • McDougall, C. J., Franklin, L. E., & Gresle, S. O. (2005). Management of radiation dermatitis in a patient after mastectomy... including commentary by Long MA. Journal of Wound, Ostomy & Continence Nursing, 32(5), 337-340. • McGowan, K. L. (1989). Radiation therapy: saving your patient's skin. RN, 52(6), 24-27. • McGowan, K. L. (2000). Additional tops for the care of irradiated skin... "Helping patients cope with skin problems caused by radiation" (Consult Stat, February). RN, 63(7), 9-9. • McQuestion, M. (2006). Evidence-based skin care management in radiation therapy. Seminars in Oncology Nursing, 22(3), 163-173. • McQuestion, M. (2011). Evidence-Based Skin Care Management in Radiation Therapy: Clinical Update. Seminars in Oncology Nursing, 27(2), e1-e17. • Meegan, M. A., & Haycocks, T. R. (1997). An investigation into the management of acute skin reactions from tangential breast irradiation. Canadian Journal of Medical Radiation Technology, 28(4), 169-173.
References • Mendelsohn, F. A., Divino, C. M., Reis, E. D., & Kerstein, M. D. (2002). Wound care after radiation therapy. Advances in Skin & Wound Care, 15(5), 216. • Miner, K. J., & Kaufman, L. M. (2011). The challenge of irradiated skin: treatment of moist desquamation using an absorbent soft silicone dressing with silver. Journal of Wound, Ostomy & Continence Nursing, 38(3S), S23-S23. • Moody, M. (2000). Study leads to development of dressings for fungating malignant wounds [commentary on Grocott P. (2000) The palliative management of fungating malignant wounds. Journal of Wound Care; 9:1, 4-9]. Nursing Times, 96(4), 17-17. • Noble-Adams, R. (1999). Clinical. Radiation-induced skin reactions 3: evaluating the RISRAS... Radiation-induced Skin Reaction Assessment Scale. British Journal of Nursing (BJN), 8(19), 1305. • Nystedt, K., Hill, J., & Mitchell, A. (2005). The stadardisation of radiation skin care in British Columbia: A collabrative approach. Oncology Nurses Forum, 32, 1199-1205. • Nystedt, K. E., Hill, J. E., Mitchell, A. M., Goodwin, F., Rowe, L. A., Wong, F. L. W., et al. (2005). The standardization of radiation skin care in British Columbia: a collaborative approach. Oncology Nursing Forum, 32(6), 1199-1205. • Porock, D., Nikoletti, S., & Kristjanson, L. (1999). Management of radiation skin reactions: literature review and clinical application. Plastic Surgical Nursing, 19(4), 185.
References • Probst, S., Arber, A., & Faithfull, S. (2009). Malignant fungating wounds: a survey of nurses' clinical practice in Switzerland. European Journal of Oncology Nursing, 13(4), 295-298. • Ratliff, C. (1990). Impaired skin integrity related to radiation therapy. Journal of Enterostomal Therapy, 17(5), 193-198. • Robson, V., & Cooper, R. (2009). Using leptospermum honey to manage wounds impaired by radiotherapy: a case series. Ostomy Wound Management, 55(1), 38. • Roy, J., & Fortin, A. (2001). The impact of skin washing with water and soap during breast irradiation: A radomized study. Journal of Radiation Oncology, 58, 333-339. • Sitton, E. (1992). Early and late radiation-induced skin alterations: nursing care of irradiated skin... part 2. Oncology Nursing Forum, 19(6), 907-912. • Smy, J. (2005). Saving their skin. Nursing Times, 101(3), 24-25. • Theberge, V., Harel, F., & Dagnault, A. (2009). Use of axillary deodarant and effect on acute skin toxicity during radiotherapy for breast cancer: A prospective randomized noninferiority trial. Journal of Radiation Oncology,Biology and Physiology, 75, 1048-1052. • Trahern, M. (2002). Aqueous cream vs baby powder: an observational study. Synergy: Imaging & Therapy Practice, 4-6. • Vavassis, P. (2008). Phase 2 study of silver leaf dressing for treatment of radiation induced dermatitis in patients recieving radiotherapy to the head and neck. Journal of Otolaryngeal Head and Neck surgery, 37, 124-129.