Download
1 / 23
230 likes | 315 Views
Promising Practices To Reduce Infant Mortality through Equity. Derek M. Griffith, Ph.D. University of Michigan Michigan Premier Public Health Conference October 12, 2011. Overview. Examine the pattern of disparities in infant mortality in Michigan

E N D
Promising Practices To Reduce Infant Mortality through Equity Derek M. Griffith, Ph.D. University of Michigan Michigan Premier Public Health Conference October 12, 2011
Overview • Examine the pattern of disparities in infant mortality in Michigan • Explore the rationale behind the PRIME Intervention strategy • Outline some of our activities, objectives, outcomes and next steps
Infant Mortality Rates by Race: United States, 1915-1997* *Note: For years 1915-1960, “White” included persons stated to be “White,” “Cuban,” “Mexican,” or “Puerto Rican.” All others during that time period were referred to as “Nonwhite.”
Black-White Ratio of Infant Mortality, U.S.: 1915-1997* YEAR *Note: For years 1915-1960, “White” included persons stated to be “White,” “Cuban,” “Mexican,” or “Puerto Rican.” All others during that time period were referred to as “Nonwhite.”
Black and White Rates of Infant Mortality in Michigan: 1970-2009 Source: 1970 - 2009 Michigan Resident Birth and Death Files, Division for Vital Records & Health Statistics, Michigan Department of Community Health
Black-White Ratio of Infant Mortality in Michigan:1970-2009 Source: 1970 - 2009 Michigan Resident Birth and Death Files, Division for Vital Records & Health Statistics, Michigan Department of Community Health
Black, Non-Hispanic Overall IMR= 14.1 Reference Overall IMR= 5.3 Maternal Health/Prematurity 7.0 Maternal Health/Prematurity 2.1 Maternal Care 1.9 Maternal Care 1.3 Newborn Care 2.0 Newborn Care 1.0 Infant Health 3.3 Infant Health 0.9 African American PPOR compared to the reference group, Michigan 2006-08 Overall Excess: 8.8 Data Source: 2008 Live Birth, Fetal Death and Death Cohort Matched Infant Death Files, Vital Records and Health Data Development Section, Michigan Department of Community Health
American Indian Overall IMR= 12.2 Reference Overall IMR= 5.3 Maternal Health/Prematurity 2.3 Maternal Health/Prematurity 2.1 Maternal Care 3.2 Maternal Care 1.3 Newborn Care 3.2 Newborn Care 1.0 Infant Health 3.6 Infant Health 0.9 American Indian PPOR compared to the reference group, Michigan 2006-08 Overall Excess: 6.9 Data Source: 2008 Live Birth, Fetal Death and Death Cohort Matched Infant Death Files, Vital Records and Health Data Development Section, Michigan Department of Community Health
PRIME Goals • Develop a training model and resources that promote understanding of practices that support institutional racism & help to eliminate racial disparities in infant mortality • Use state/local partnership network to codify effective efforts that undo racism & help to eliminate racial disparities in infant mortality • Establish a sustainable quality assurance process for these efforts within the BFMCH
PRIME Funding and Structure • Kellogg awarded one-year grant • May 2010 • Kellogg awarded 2 additional years • December 2010 • Steering Team • Intervention Workgroup • Evaluation Workgroup • Local Learning Collaborative
Public Health Administration J. Chabut B. Pash FMCH Bureau A. Carr B. Jegede C. Ogan B. Fink P. Dobynes-Dunbar C. Celestin L. Barnett B. Pash S. Bien Epidemiology B. Coughlin PRIME Steering Team • Minority Health Section • S. Weir • H. Nichol • University of Michigan • D. Griffith • J. Ober Allen • T. Reischl • Local Public Health • R. Canady • Hammami • CBO • E. Clement • E. Kushman • L. Abramson • D. Peterson
Local Learning Collaborative • Healthy Start Programs • Detroit • Genesee • Grand Rapids • Kalamazoo • Native American (Sault Ste. Marie) • Saginaw • Community-based Organizations • ACCESS, Dearborn • Dispute Resolution Center, Ann Arbor • Grand Rapids African American Health Initiative • MI Minority Health Coalition • National Kidney Foundation • MI Department of Community Health • County/City Health Departments • Berrien County • Detroit • Genesee County • Ingham County • Jackson County • Kalamazoo County • Kent County • Oakland County • Washtenaw County
Conceptual • Individual (risk factors) vs. Population Health approach • Make explicit and plain what SDOH mean for how we think about racial disparities • Incorporate social and cultural assets • Unique social, cultural and historical roots of racial disparities - AA-White and AI-White
Practical • Develop and pilot resources and experiences that help staff incorporate SDOH in their day-to-day work • Create tools that promote staff accountability and increase staff capacity to attend to SDOH • Increase the capacity of staff and teams to assess and address their training needs in these areas
Technical • Create separate but complementary plans to address AA-White and AI-White disparities in infant mortality • Improve the quality of data available to inform statewide strategies to address AA-White and AI-White disparities in infant mortality • Increase capacity for BFMCH for staff to use data to inform decisions, practices and policies
Organizational • Revise strategic plans and other documents • Decrease duplication of BFMCH and MDCH programs that affect infant mortality • More effective utilization of inter-division expertise, resources and data and better quality improvement • Increase capacity for BFMCH to support local efforts to address racial disparities in infant mortality
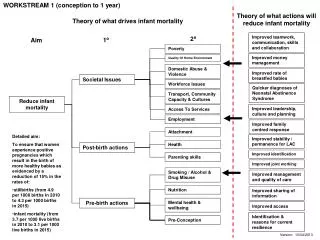
Promising Practices To Reduce Infant Mortality through Equity Principal Investigator, Alethia Carr INPUTS ACTIVITIES OUTPUTS OUTCOMES Evaluation • Contextual Conditions • >20 year disparity in infant mortality in MI • MI economic challenges • Decreasing MDCH budget • large percentage of MDCH staff are eligible for retirement Recruit & hire project coordinator & leadership team to lead bureau efforts • Project coordinator • # of leadership team meetings • Meeting minutes • # of leaders involved in meetings and training activities • Short-Term Outcomes • Increased Knowledge of Staff • Tool kit & curriculum • Change in BFMCH policies that may contribute to the racial disparity in IM • Increased monitoring of SDOH in statewide health disparity report • Increased continuous quality improvement and public sharing of measurable outcomes that reflect racial equity and health equity • Increased BFMCH-local partnership efforts to reduce racial disparities in IM Review of bureau and non-health policies and practices • # of meetings or discussions devoted to Bureau Review activity • # of participants involved in meetings and training activities • # of Employee Hours devoted to project activities Conduct self-assessment of MDCH social justice orientation • Human Resources • Leadership of MCH Bureau Director • Co-Investigator and Evaluator from UMSPH • Collaborators: NACCHO, local health officials, & MDCH directors & staff • External training consultants, content experts, contractors & facilitators Review of existing models and curricula Create tool kit and curriculum on social determinants of racial disparities • Documents • Epidemiologic report to monitor IM disparities • Green paper review of possible intervention strategies • White paper of new policies & guidelines • Distribution of Green and White papers to key people for feedback Write and get expert feedback on reports, green paper, & white paper • Long-Term Goal • Reduction in the black/ white racial disparity in infant mortality in MI Opportunities for Inter- & Intra-departmental collaboration (i.e., HDRMH, DHS, Medicaid, etc.) Staff training Revised, June 17, 2009
“The aim of research on health disparities is not to just accurately describe health differences or determine their cause, but to do so in a way that will be useful to making predictions, preventing greater health disparities, and improving human health.” (de Melo-Martin & Intemann, 2007)
Poverty Thresholds 2006 (Use landscape & legal printer options to print this table) Derek M. Griffith, Ph.D. derekmg@umich.edu University of Michigan School of Public Health