Download
1 / 1
10 likes | 73 Views
Explore how depressive mood is associated with natural mortality, considering gender differences and specific causes of death. This large-scale prospective study in France analyzes the impact of depressive mood on mortality rates.

E N D
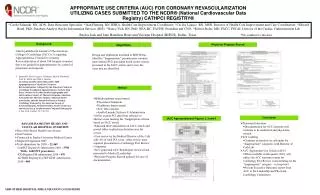
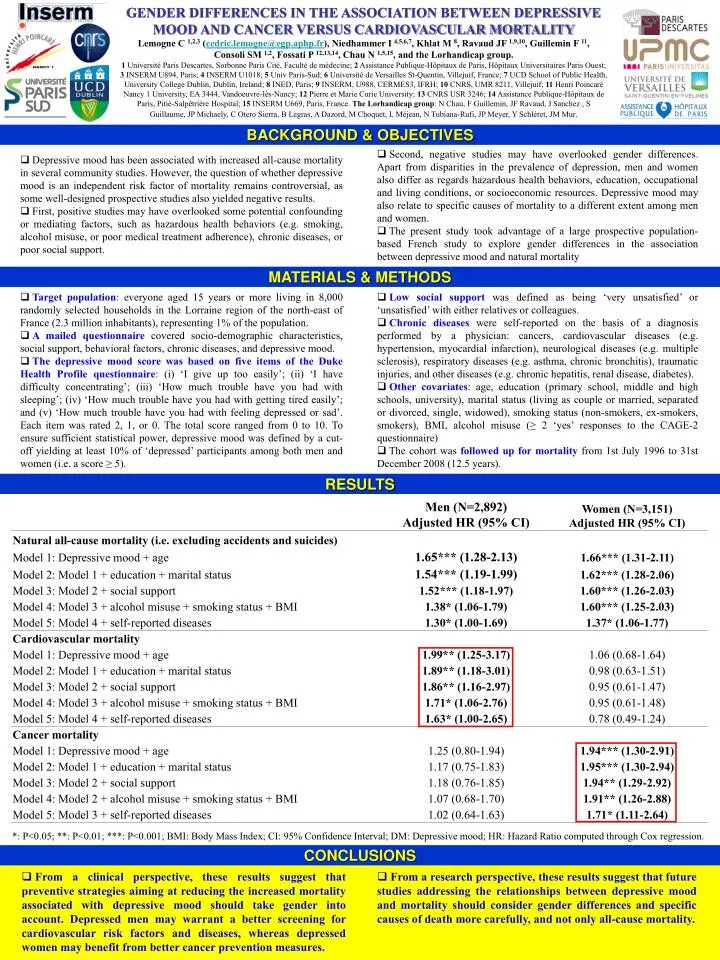
GENDER DIFFERENCES IN THE ASSOCIATION BETWEEN DEPRESSIVE MOOD AND CANCER VERSUS CARDIOVASCULAR MORTALITY Lemogne C 1,2,3(cedric.lemogne@egp.aphp.fr), Niedhammer I 4,5,6,7, Khlat M 8, Ravaud JF 1,9,10, Guillemin F 11, Consoli SM 1,2, Fossati P 12,13,14, Chau N 1,5,15, and the Lorhandicap group. 1 Université Paris Descartes, Sorbonne Paris Cité, Faculté de médecine; 2 Assistance Publique-Hôpitaux de Paris, Hôpitaux Universitaires Paris Ouest; 3 INSERM U894, Paris; 4 INSERM U1018; 5 Univ Paris-Sud; 6 Université de Versailles St-Quentin, Villejuif, France; 7 UCD School of Public Health, University College Dublin, Dublin, Ireland; 8 INED, Paris; 9 INSERM, U988, CERMES3, IFRH; 10 CNRS, UMR 8211, Villejuif; 11 Henri Poincaré Nancy 1 University, EA 3444, Vandoeuvre-lès-Nancy; 12 Pierre et Marie Curie University; 13 CNRS USR 3246; 14 Assistance Publique-Hôpitaux de Paris, Pitié-Salpêtrière Hospital; 15 INSERM U669, Paris, France. The Lorhandicap group: N Chau, F Guillemin, JF Ravaud, J Sanchez , S Guillaume, JP Michaely, C Otero Sierra, B Legras, A Dazord, M Choquet, L Méjean, N Tubiana-Rufi, JP Meyer, Y Schléret, JM Mur. BACKGROUND & OBJECTIVES • Depressive mood has been associated with increased all-cause mortality in several community studies. However, the question of whether depressive mood is an independent risk factor of mortality remains controversial, as some well-designed prospective studies also yielded negative results. • First, positive studies may have overlooked some potential confounding or mediating factors, such as hazardous health behaviors (e.g. smoking, alcohol misuse, or poor medical treatment adherence), chronic diseases, or poor social support. • Second, negative studies may have overlooked gender differences. Apart from disparities in the prevalence of depression, men and women also differ as regards hazardous health behaviors, education, occupational and living conditions, or socioeconomic resources. Depressive mood may also relate to specific causes of mortality to a different extent among men and women. • The present study took advantage of a large prospective population-based French study to explore gender differences in the association between depressive mood and natural mortality MATERIALS & METHODS • Target population: everyone aged 15 years or more living in 8,000 randomly selected households in the Lorraine region of the north-east of France (2.3 million inhabitants), representing 1% of the population. • A mailed questionnaire covered socio-demographic characteristics, social support, behavioral factors, chronic diseases, and depressive mood. • The depressive mood score was based on five items of the Duke Health Profile questionnaire: (i) ‘I give up too easily’; (ii) ‘I have difficulty concentrating’; (iii) ‘How much trouble have you had with sleeping’; (iv) ‘How much trouble have you had with getting tired easily’; and (v) ‘How much trouble have you had with feeling depressed or sad’. Each item was rated 2, 1, or 0. The total score ranged from 0 to 10. To ensure sufficient statistical power, depressive mood was defined by a cut-off yielding at least 10% of ‘depressed’ participants among both men and women (i.e. a score ≥ 5). • Low social support was defined as being ‘very unsatisfied’ or ‘unsatisfied’ with either relatives or colleagues. • Chronic diseases were self-reported on the basis of a diagnosis performed by a physician: cancers, cardiovascular diseases (e.g. hypertension, myocardial infarction), neurological diseases (e.g. multiple sclerosis), respiratory diseases (e.g. asthma, chronic bronchitis), traumatic injuries, and other diseases (e.g. chronic hepatitis, renal disease, diabetes). • Other covariates: age, education (primary school, middle and high schools, university), marital status (living as couple or married, separated or divorced, single, widowed), smoking status (non-smokers, ex-smokers, smokers), BMI, alcohol misuse (≥ 2 ‘yes’ responses to the CAGE-2 questionnaire) • The cohort was followed up for mortality from 1st July 1996 to 31st December 2008 (12.5 years). RESULTS *: P<0.05; **: P<0.01; ***: P<0.001; BMI: Body Mass Index; CI: 95% Confidence Interval; DM: Depressive mood; HR: Hazard Ratio computed through Cox regression. CONCLUSIONS • From a clinical perspective, these results suggest that preventive strategies aiming at reducing the increased mortality associated with depressive mood should take gender into account. Depressed men may warrant a better screening for cardiovascular risk factors and diseases, whereas depressed women may benefit from better cancer prevention measures. • From a research perspective, these results suggest that future studies addressing the relationships between depressive mood and mortality should consider gender differences and specific causes of death more carefully, and not only all-cause mortality.