Download

1 / 23
240 likes | 481 Views
Palpitations in primary care- InnovAit, July 2011. Aisha Bhaiyat. Aim. Assessment Management ECG’s. Palpitations. Prevalence – 16% of primary care consultations 2 nd commonest reason for gp referral to cardiology. Assessment. What does the patient mean by palpitation Rate Rhythm

E N D
Palpitations in primary care- InnovAit, July 2011 Aisha Bhaiyat
Aim • Assessment • Management • ECG’s
Palpitations • Prevalence – 16% of primary care consultations • 2nd commonest reason for gp referral to cardiology
Assessment • What does the patient mean by palpitation • Rate • Rhythm • Missed/extra beat • Associated symptoms • Onset/offset • Exacerbating/relieving • Timings
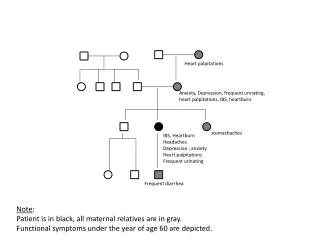
Assessments • Past medical history • Drug history • Family history • Social history • Examination
Medical emergency • Systolic BP less than 90 mmHg • Pulse less than 40 or greater than 150 • Cardiac failure • Chest pain • Presyncope
Management • ECG • Blood tests • Ambulatary ECG • Transthoracic echo – if structural cardiac abnormality suspected
ECG abnormalities that may be present in those with palpitations Conduction abnormalities Structural heart disease related LVH T wave/ST changes Features of old MI • BBB • Venricular pre-excitation • Prolongue QTc • Extreme 1st degree block • 2nd/3rd degree block • Other arrythmias eg AF
Red Flags/high risk-urgent referral to cardiology • Exercise related palpitations • Syncope/presyncope • FH of sudden cardiac death/inherited heart dx • ECG-high degree av block • High risk structural disease
Amber Flags/moderate risk-refer to cardiology • History suggestive of recurrent tachyarrythmia • Palpitation with associated symptoms • Abnormal ECG (other than high av block) • Structural heart disease
Low risk-manage in primary care • Skipped or thumping beats • Slow pounding sensation • ECG normal • No structural heart disease
Management and referral pathway for patients presenting with palpitations. Taggar J S , Hodson A, The assessment and management of palpitations in primary care InnovAiT 2011;4(7):408-413, By permission of oxford university press.
Further considerations • Opportunistic health promotion • Driving – must cease if arrythmia likely to cause incapacity. Permitted once arrythmia identified and controlled for 4/52. DVLA need to be indentified only symptoms are disabling • Occupation • Genetics-HOCM, WPW, Brugada syndrome, Long QTS
Key points • Consider lifestyle/psychological/other systemic medical causes • After initial assessment, patients risk should be stratified and managed appropriately • Other considerations - health promotion/ driving/occupation/genetics
Useful websites • Heart Rhythm UK [www.hruk.org.uk/] • Arrhythmia Alliance [www.heartrhythmcharity.org.uk/] (most useful for patient information leaflets) • Sudden Adult Death Trust [www.sadsuk.org/] • Cardiac risk in the young [www.c-r-y.org.uk/]