Download
1 / 48
550 likes | 1.47k Views
FNA of the Pancreas. David Kindelberger, MD Divisions of Cytopathology and Women’s and Perinatal Pathology, Department of Pathology, Brigham and Women’s Hospital. Financial Disclosures.

E N D
FNA of the Pancreas David Kindelberger, MD Divisions of Cytopathology and Women’s and Perinatal Pathology, Department of Pathology, Brigham and Women’s Hospital
Financial Disclosures • Dr. Kindelberger has no relationships to commercial interests relating to the content of this presentation.
Oncologic History 59 year old woman 10/04: RUQ pain radiating to R flank, decreased appetite, early satiety, diarrhea followed by pale stools/dark urine 11/04: Abd CT showed 3x3 cm mass in head of pancreas with both intra and extra-hepatic BDD 12/04: ERCP with EUS (+FNA) showed hypoechoic mass in pancreatic head with probable portal vein invasion. FNA performed. Sphincterotomy performed and stent placed
Cytologic Diagnosis • POSITIVE FOR MALIGNANT CELLS • Consistent with adenocarcinoma
Oncologic History (cont.) 1/05-2/05: XRT 1/05: Begin concurrent CI 5-FU, CEA 11.9, CA19-9 1346 3/05: Abd CT showed multiple liver lesions and increasing size of pancreatic mass. CA19-9 5403 4/05: Increasing N/V with worsening fatigue and elevated LFTs
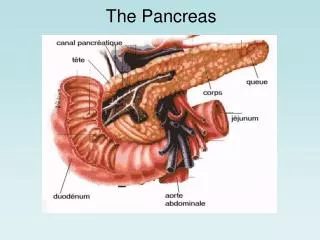
Endoscopic Ultrasound Guided FNA of the Pancreas • Introduction • Solid Lesions • Cystic Lesions • Conclusions
Introduction • 1851 Lebert was among the first to publish on using “percutaneous tumor puncture” • 1966 Dahlgren and Nordenstrom first reported using FNA of lung tumors under fluoroscopy • 1970 Oscarson used selective angiography to guide percutaneous biopsy of the pancreas • 1975 Smith used US guidance for percutaneous biopsy of the pancreas • 1982 Endoscopic ultrasonography introduced • 1992 Vilmann used endoscopic ultrasound to guide FNA of the pancreas.
Advantages of EUS-Guided FNA • Allows for biopsy of smaller lesions (lesions less than 0.5 cm have been accurately biopsied) • Much shorter needle path (only pass through gastric or duodenal wall) • Can be performed at time of initial staging
Disadvantages of EUS-Guided FNA • Risks associated with endoscopy/conscious sedation • Time consuming (1-1.5 hours per procedure) • Results highly dependent on level of operator and cytology experience
Sensitivity and Specificity • Large series (179 cases) from MD Anderson • Sensitivity: 83.5 % • Specificity: 100% (also 100% PPV) • Diagnostic accuracy: 80.3% (using resection as gold standard in 70 cases)
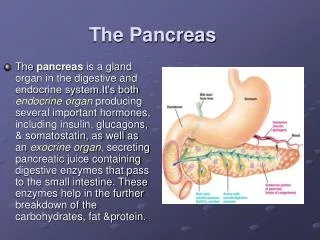
Ductal Adenocarcinoma • 85-90% of pancreatic neoplasms • Incidence rates in developed countries range from 3 to 20 per 100,000 males (incidence and mortality almost identical) • 5th leading cause of cancer death in Western countries • Over 80% of cases present between 60-80 yrs. old • Male/female = 1.6
Ductal Adenocarcinoma • Risk Factors • Smoking • Chronic pancreatitis • Past gastric surgery • Diabetes • Chlorinated hydrocarbons • Location • 60-70% found in head (mainly in upper half)
Ductal Adenocarcinoma • Diagnostic Approaches • US or CT/MRI • Tumor markers (CA19-9, CEA, etc) • EUS-guided FNA
Variants of Ductal Adenocarcinoma • Adenosquamous carcinoma • Undifferentiated (Giant Cell) carcinoma • Mucinous, non-cystic carcinoma • Signet-ring cell carcinoma • Undifferentiated carcinoma with osteoclast-like giant cells • Mixed ductal-endocrine carcinoma
Ductal Adenocarcinoma • Poor Prognosis: • Mean untreated survival time is 3 months • Mean survival time (after radical resection) is 10-20 months • Overall 5 year survival is 3-4%
Acinar Cell Carcinoma • 1-2% of exocrine pancreatic neoplasms • Most occur in older patients (mean age = 62) • Male:Female 2 • 10-15% of patients develop lipase hypersecretion syndrome (subcutaneous fat necrosis with polyarthralgia)
Acinar Cell Carcinoma • Immunostains for pancreatic enzymes may be helpful (esp trypsin and chymotrypsin) • Poor Prognosis: • Median survival time is 8 months • Overall 5 year survival is <10% (particularly short in pts. with lipase hypersecretion syndrome)
Solid Pseudopapillary Tumor • 1-2% of pancreatic exocrine tumors • Predominantly in adolescent and young adult women (mean age = 35); rare in men • Etiology unknown • Typically found incidentally
Histology of Solid Pseudopapillary Tumor Resection Specimen PAS Stain
Solid Pseudopapillary Tumor • Immunostains for a-1-antitrypsin, a-1-antichymotrypsin, b-catenin, and vimentin may be helpful • Very good prognosis • >95% survival following complete resection • Local spread within peritoneal cavity and rare deaths from metastatic disease have ben reported
Pancreatic Endocrine Neoplasms • 1-5% of pancreatic neoplasms • Often occur in middle-aged adults (mean age 55-60) • Many present with symptoms related to hormone production by tumors
Pancreatic Endocrine Neoplasms • Immunostains for chromogranin, synaptophysin, and specific hormone products may be helpful • Variable prognosis
Cystic Neoplasms of the Pancreas • Must integrate diagnostic modalities • Imaging • Cyst fluid chemistry • Cyst aspiration cytology • Three main questions must be answered • Pseudocyst vs. Neoplastic cyst? • If neoplastic, is it serous or mucinous? • If mucinous, is it malignant?
Serous Cystadenoma • Most common true cystic tumor of pancreas • Usually microcystic • F>M (median age = 66 • Pts. With VHL have similar appearing cysts)
Serous Cystadenoma • Immunostains for keratins, EMA, MART-1 may be helpful • Are benign neoplasms
Mucinous Cystic Neoplasm • Second most common cystic tumor of pancreas • Usually macrocystic • F>>>>>>>>>>>M (median age = 50) • No communication with pancreatic duct • Presence of ovarian-type stroma
Mucinous Cystic Neoplasm • Immunostains for EMA, and CEA (epithelial components) or SMA, vimentin, desmin (stromal components) may be helpful • Prognosis is excellent if tumor completely resected
Summary • EUS alone is very sensitive (80-90%)—particularly well suited for small lesions—but not specific (53%) • When combined with FNA, sensitivity remains high (80-90%) and specificity approaches 100% • EUS guided FNA has greater sensitivity, specificity, and negative predictive value than CT guided biopsy