Download
1 / 1
50 likes | 408 Views
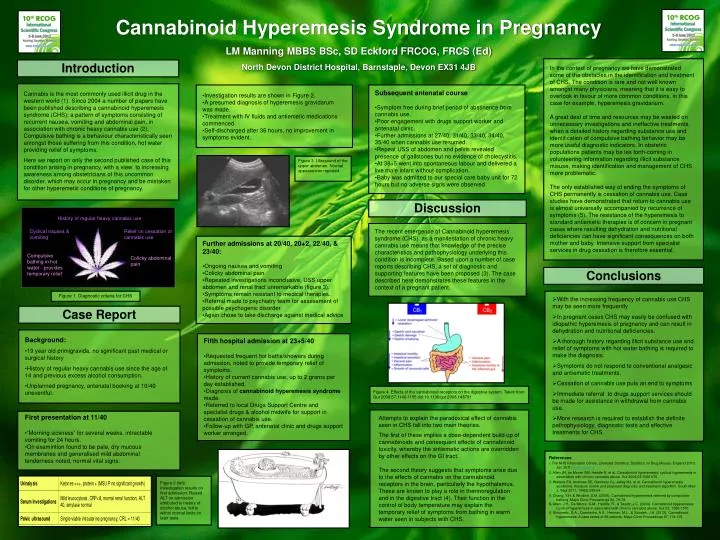
History of regular heavy cannabis use. Cyclical nausea & vomiting. Relief on cessation of cannabis use. Compulsive bathing in hot water - provides temporary relief. Colicky abdominal pain. Cannabinoid Hyperemesis Syndrome in Pregnancy LM Manning MBBS BSc, SD Eckford FRCOG, FRCS (Ed)

E N D
History of regular heavy cannabis use Cyclical nausea & vomiting Relief on cessation of cannabis use Compulsive bathing in hot water - provides temporary relief Colicky abdominal pain Cannabinoid Hyperemesis Syndrome in Pregnancy LM Manning MBBS BSc, SD Eckford FRCOG, FRCS (Ed) North Devon District Hospital, Barnstaple, Devon EX31 4JB Introduction In the context of pregnancy we have demonstrated some of the obstacles in the identification and treatment of CHS. The condition is rare and not well known amongst many physicians, meaning that it is easy to overlook in favour of more common conditions, in this case for example, hyperemesis gravidarium. A great deal of time and resources may be wasted on unnecessary investigations and ineffective treatments, when a detailed history regarding substance use and identification of compulsive bathing behavior may be more useful diagnostic indicators. In obstetric populations patients may be les forth-coming in volunteering information regarding illicit substance misuse, making identification and management of CHS more problematic. The only established way of ending the symptoms of CHS permanently is cessation of cannabis use. Case studies have demonstrated that return to cannabis use is almost universally accompanied by recurrence of symptoms (5). The resistance of the hyperemesis to standard antiemetic therapies is of concern in pregnant cases where resulting dehydration and nutritional deficiencies can have significant consequences on both mother and baby. Intensive support from specialist services in drug cessation is therefore essential. • Subsequent antenatal course • Symptom free during brief period of abstinence from cannabis use. • Poor engagement with drugs support worker and antenatal clinic. • Further admissions at 27/40, 31/40, 33/40, 34/40, 35/40 when cannabis use resumed. • Repeat USS of abdomen and pelvis revealed presence of gallstones but no evidence of cholecystitis. • At 38+5 went into spontaneous labour and delivered a live male infant without complication. • Baby was admitted to our special care baby unit for 72 hours but no adverse signs were observed • Investigation results are shown in Figure 2. • A presumed diagnosis of hyperemesis gravidarum was made. • Treatment with IV fluids and antiemetic medications commenced. • Self-discharged after 36 hours, no improvement in symptoms evident. Cannabis is the most commonly used illicit drug in the western world (1). Since 2004 a number of papers have been published describing a cannabinoid hyperemesis syndrome (CHS); a pattern of symptoms consisting of recurrent nausea, vomiting and abdominal pain, in association with chronic heavy cannabis use (2). Compulsive bathing is a behaviour characteristically seen amongst those suffering from this condition, hot water providing relief of symptoms. Here we report on only the second published case of this condition arising in pregnancy, with a view to increasing awareness among obstetricians of this uncommon disorder, which may occur in pregnancy and be mistaken for other hyperemetic conditions ofpregnancy. Figure 3. Ultrasound of the upper abdomen. Normal appearances reported. Discussion The recent emergence of Cannabinoid hyperemesis syndrome (CHS) as a manifestation of chronic heavy cannabis use means that knowledge of the precise characteristics and pathophysiology underlying this condition is incomplete. Based upon a number of case reports describing CHS, a set of diagnostic and supporting features have been proposed (3). The case described here demonstrates these features in the context of a pregnant patient. • Further admissions at 20/40, 20+2, 22/40, & 23/40: • Ongoing nausea and vomiting • Colicky abdominal pain • Repeated investigations inconclusive, USS upper abdomen and renal tract unremarkable (figure 3). • Symptoms remain resistant to medical therapies. • Referral made to psychiatry team for assessment of possible psychogenic disorder. • Again chose to take discharge against medical advice Conclusions Figure 1. Diagnostic criteria for CHS • With the increasing frequency of cannabis use CHS may be seen more frequently • In pregnant cases CHS may easily be confused with idiopathic hyperemesis of pregnancy and can result in dehydration and nutritional deficiencies. • A thorough history regarding illicit substance use and relief of symptoms with hot water bathing is required to make the diagnosis. • Symptoms do not respond to conventional analgesic and antiemetic treatments. • Cessation of cannabis use puts an end to symptoms • Immediate referral to drugs support services should be made for assistance in withdrawal from cannabis use. • More research is required to establish the definite pathophysiology, diagnostic tests and effective treatments for CHS. Case Report • Background: • 19 year old primigravida, no sginificant past medical or surgical history • History of regular heavy cannabis use since the age of 14 and previous excess alcohol consumption. • Unplanned pregnancy, antenatal booking at 10/40 uneventful. • Fifth hospital admission at 23+5/40 • Requested frequent hot baths/showers during admission, noted to provide temporary relief of symptoms. • History of current cannabis use, up to 2 grams per day established. • Diagnosis of cannabinoid hyperemesis syndrome made. • Referred to local Drugs Support Centre and specialist drugs & alcohol midwife for support in cessation of cannabis use. • Follow-up with GP, antenatal clinic and drugs support worker arranged. Figure 4. Effects of the cannabinoid receptors on the digestive system. Taken from Gut 2008;57:1140-1155 doi:10.1136/gut.2008.148791 • First presentation at 11/40 • “Morning sickness” for several weeks, intractable vomiting for 24 hours. • On examintion found to be pale, dry mucous membranes and generalised mild abdominal tenderness noted, normal vital signs. Attempts to explain the paradoxical effect of cannabis seen in CHS fall into two main theories. The first of these implies a dose-dependent build up of cannabinoids and consequent effects of cannabinoid toxicity, whereby the antiemetic actions are overridden by other effects on the GI tract. The second theory suggests that symptoms arise due to the effects of cannabis on the cannabinoid receptors in the brain, particularly the hypothalamus. These are known to play a role in thermoregulation and in the digestive tract (4). Their function in the control of body temperature may explain the temporary relief of symptoms from bathing in warm water seen in subjects with CHS. References 1. The NHS Information Centre, Lifestyles Statistics. Statistics on Drug Misuse: England 2010. Jan 2011; www.ic.nhs.uk 2. Allen JH, de Moore GM, Heddle R, et al. Cannabinoid hyperemesis: cyclical hyperemesis in association with chronic cannabis abuse. Gut 2004;53:1566 ñ70. 3. Wallace EA, Andrews SE, Garmany CL, Jelley MJ, et al. Cannabinoid hyperemesis syndrome: literature review and proposed diagnosis and treatment algorithm. South Med J, Sept 2011; 104(9):659-64. 4. Chang, Y.H. & Windish, D.M. (2009). Cannabinoid hyperemesis relieved by compulsive bathing. Mayo Clinic Proceedings 84, 76-78. 5. Allen, J.H., De Moore, G.M., Heddle, R., & Twartz, J.C. (2004). Cannabinoid hyperemesis: Cyclical hyperemesis in associationwith chronic cannabis abuse. Gut 53, 1566-1570. 6. Simonetto, D.A., Oxentenko, A.S., Herman, M.L., & Szostek, J.H. (2012). Cannabinoid hyperemesis: A case series of 98 patients. Mayo Clinic Proceedings 87, 114-119. Figure 2 (left). Investigation results on first admission. Raised ALT on admission attributed to history of alcohol abuse, fell to within normal limits on later tests.