Download

1 / 51
510 likes | 717 Views
Role of surgery in treatment of fecal incontinence disorders. Rasoul Azizi M.D Colo-Rectal Surgeon Associate Professor of surgery School of Medical Sciences , Tehran University Rasoul Akram Medical Complex Tehran- Iran E- mail: razizimd@hotmail.com.

E N D
Role of surgery in treatment of fecal incontinence disorders Rasoul Azizi M.D Colo-Rectal Surgeon Associate Professor of surgery School of Medical Sciences, Tehran University Rasoul Akram Medical Complex Tehran- Iran E- mail: razizimd@hotmail.com
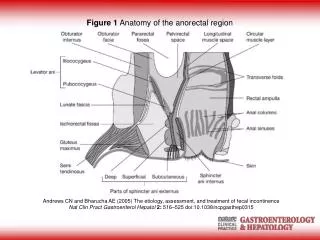
Factors contribute to the ability to control feces The consistency of the feces is important The peristalsis in rectosigmoid has a role in keeping the rectum empty. The rectal capacity is important to store feces for some time. The pelvic floor muscles are of help to form a barrier when they are contracted. The internal anal sphincter is contracted and gives watertight closure of the anal canal with the help of hemorrhoidal tissue. Contraction of the external sphincter as additional help to internal sphincter. The central nervous system has to govern the sensoric input and the motoric output.
All these factors form a delicate system to keep the human continent.When something goes wrong in one these factors, it is depending on the quality of the other factors whether this lead to incontinence.
Symptoms Fecal incontinence is a frequent problem but very much underreported because of embarrassment. It is devastating disorder, which affect 2.2% community-dwelling adults and 45% of nursing home residents. Fecal incontinence forms the most important reason to place patients in a nursing home. In FI the compliant is often not directly voiced. The psychologic impact is devastating. They often conceal their problems by complaining of chronic diarrhea, defecation problems or rectal urgency. A thorough history is therefore essential in assessing patients with FI
Causes of Incontinence 1-Congenital 2- Pelvic floor Denervation 3- Obstetric 4- Iatrogenic 5- Traumatic 6- Radiation
Treatment Conservative treatment Biofeedback Balloon Training Electrostimulation
Sphincteroplasty Obstetrical trauma Fistulotomy Sphincterotomy Hemorrhoidectomy Localized external trauma
Indications Post anal repair is currently performed on patients with idiopathic fecal incontinence with no evidence of sphincter defect. The patients expected to benefit most from post anal repair are women with a history of multiple vaginal deliveries.
Dynamic GraciloplastyIndications Restoration of the sphincters after rupture due to obstetric causes. Impalement trauma of the perineum. Complications of perineal operations
Results Several series have been published that indicate success rates from 45% to 80% However, and many complications have been reported. Infection – Constipation- Insufficient contraction of gracilis.
The Artificial Bowel Sphincter The ABS functions semi automatically Defecation is initiated by the patient Anal closure occurs again automatically in 5-8 min by passive fluid transfer and a progressive return to baseline pressure in the cuff.
Recently published Results withABS The overall incidence of permanent explanation of the ABS in the published series varied between 17% and 31% with follow up periods of between 10 and 58 months. Revision surgery with replacement of part of or the entire device occurred in between 7% and 25% of patients.
Complication Perioperative infections Failure of wound healing Erosion of part of the device through the skin or the anal canal. Late infection. Mechanical malfunction of the device due to cuff or balloon rupture.
Gluteoplastysurgical approach and operative technique Preoperative evaluation includes assessment by multidisplinary team that comprises members from general or colo-rectal surgery, plastic surgery, urogynecology and gastroentrology. Workup involves: sigmoidoscopy, endorectal ultrasound, rectal manometry, and pudental nerve studies
Sacral Nerve Stimulation Temporary, percutaniously placed, test stimulation lead. Permanent system consisting of an electrode, connecting cable and pulse generator.
Injectable Bulking Agents In, 1938 obstetric registrar used paraurethral injection of sodium morrhaute to stimulate the formation of fibrous tissue. Since, 1964, urologists have also used injectable bulking agents to close down the bladder neck In, 1993, Polytetrafluoroethylene(Tetron or Polytef) injected to anal submucosa for FI
The Injectable Bulking Agents In broad terms, an agents should be: Biocompatible Nonmigratory Non allergic Nonimmunogenic Non-carcinogenic Easy to inject Able to produce durable results
RadiofrequencySecca procedure This procedure is not an option for obvious sphincter defects but can be used with a weak or thinned anal sphincter complex. Patients with history of IBD, extensive perianal disease, or chronic diarrhea should not be offered this treatment.
FI in elderly and Institutionalized Patients Prevalence: Age more than 65 years 3.7-27% Hospitalized patients 10-25% Nursing home > 50% Hospitalization with dementia > 80%
Double Incontinence A significant association between urinary and anal incontinence was found in patients with pelvic floor disorders This association was found in women with concomitant UI and pelvic organ prolapse who have higher incidence of anal incontinence