Download
1 / 32
320 likes | 631 Views
Chapter 15 Subtypes of Primary Speech Sound Disorders: Theories and Case Studies. Beate Peter. Classification in General. Creating groups Similar within groups Dissimilar among groups Examples: clothes in your closet, bins at the bead store, grocery shelves, library books,

E N D
Chapter 15Subtypes of Primary Speech Sound Disorders: Theories and Case Studies Beate Peter
Classification in General • Creating groups • Similar within groups • Dissimilar among groups • Examples: clothes in your closet, bins at the bead store, grocery shelves, library books, • Taxonomies (plants, animals) • Nosologies (diseases) 1.thesystematicclassification of diseases. 2. the knowledge of a disease. • Sometimes, multiple solutions are possible • Different ways to classify plants and animals • Different library catalog systems • Different classifications of diseases in the Diagnostic and Statistical Manual (DSM) and International Classification of Diseases (ICD)
Why an Accurate Nosology Matters for Speech Sound Disorders Evidence-based practice Diagnostic label Prognosis Selection of treatment approach Example: subtype of dystonia that responds to levadopa.
A Few Definitions • Speech sound disorder • With a known cause, for example • Structural anomalies such as cleft lip and/or palate • Developmental disabilities such as trisomy 21 • Hearing impairment • Motor impairments such as dysarthria secondary to cerebral palsy • Without a known cause • Error types • Distortion (slight change; target sound easily recognizable) – examples are lisps or clear instead of dark /l/ sounds • Omissions, for instance in cluster reductions • Insertions, for instance in epenthesis • Substitutions, for instance w/r, t/k
Proposed Nosologies for Speech Sound Disorders Articulation, e.g., lateral lisp Phonology, e.g., final obstruent deletion 15S1 Story retell provided by a boy, age 5;0, with a lateral lisp 15S2 Picture naming provided by a girl, age 4;11, with multiple phonological processes Jaqueline Bauman-Waengler: Continuum from articulation to phonology
Phonology Articulation (consistent mispronunciation or distortion in all phonetic contexts) Delayed Disordered Inconsistent Consistent Barbara Dodd: Error types
Shriberg et al. (2010) • Typology (grouped by observable traits) • Normal Speech Acquisition • Speech Delay: speech sound deletions, substitutions, and distortions that usually respond to treatment. • Motor Speech Disorder: speech sound deletions, substitutions, and distortions may not completely normalize with treatment. • Speech Errors: speech sound distortions such as sibilants and/or liquids. • Etiology (grouped by suspected causes) • genetic and environmental influences on neurodevelopmental substrates • Cognitive-linguistic etiology: Speech Delay – Generic • Auditory-perceptual: Speech Delay – Otitis Media with Effusion • Psychosocial: Speech Delay – Developmental Psychosocial Involvement • Speech motor control: Motor Speech Disorder • Apraxiaof speech • Dysarthria • not otherwise specified • Speech attunement: Speech Errors related to distortions of • Sibilants • Rhotics
“[CAS] is a neurological childhood (pediatric) speech sound disorder in which the precision and consistency of movements underlying speech are impaired in the absence of neuromuscular deficits (e.g., abnormal reflexes, abnormal tone). CAS may occur as a result of known neurological impairment, in association with complex neurobehavioral disorders of known or unknown origin, or as an idiopathic neurogenic speech sound disorder. The core impairment in planning and/or programming spatiotemporal parameters of movement sequences results in errors in speech sound production and prosody.” American Speech-Language-Hearing Association http://www.asha.org/docs/html/PS2007-00277.html Childhood apraxia of speech
What are some signs or symptoms of childhood apraxia of speech? http://www.asha.org/public/speech/disorders/childhoodapraxia.htm A Very Young Child Does not coo or babble as an infant First words are late, and they may be missing sounds Only a few different consonant and vowel sounds Problems combining sounds; may show long pauses between sounds Simplifies words by replacing difficult sounds with easier ones or by deleting difficult sounds (although all children do this, the child with apraxia of speech does so more often) May have problems eating
http://www.asha.org/public/speech/disorders/childhoodapraxia.htmhttp://www.asha.org/public/speech/disorders/childhoodapraxia.htm An Older Child Makes inconsistent sound errors that are not the result of immaturity Can understand language much better than he or she can talk Has difficulty imitating speech, but imitated speech is more clear than spontaneous speech May appear to be groping when attempting to produce sounds or to coordinate the lips, tongue, and jaw for purposeful movement Has more difficulty saying longer words or phrases clearly than shorter ones Appears to have more difficulty when he or she is anxious Is hard to understand, especially for an unfamiliar listener Sounds choppy, monotonous, or stresses the wrong syllable or word
http://www.asha.org/public/speech/disorders/childhoodapraxia.htmhttp://www.asha.org/public/speech/disorders/childhoodapraxia.htm Potential Other Problems Delayed language development Other expressive language problems like word order confusions and word recall Difficulties with fine motor movement/coordination Over sensitive (hypersensitive) or under sensitive (hyposensitive) in their mouths (e.g., may not like toothbrushing or crunchy foods, may not be able to identify an object in their mouth through touch) Children with CAS or other speech problems may have problems when learning to read, spell, and write
15S3 Conversational speech of a girl with a CAS diagnosis, age 3;2 15S4 Articulation test of a girl with a CAS diagnosis, age 5;11
15S5 Single words (“spoon,” “girl,” “ball,” “wagon,” “shovel”) produced by a 10-year-old boy with dysarthria • Dysarthria • Unlike SSD and CAS, there can be a known etiology • Caused by impairments in the central or peripheral nervous system • Speech is affected because of impairments at the level of muscular control
Psycholinguistic models (Stackhouse & Pascoe, 2010; Stackhouse & Wells, 1997) • Focus is on underlying deficit rather than speech behaviors • Input-related processes, e.g. • Peripheral auditory perception • Speech/nonspeechdiscrimination • Phonological recognition • Elements of stored knowledge, e.g. • Phonological representation • Semantic representation • Output-related processes, e.g. • Motor planning • Motor execution. • Breakdowns can occur in any of these components and cause speech problems • Psycholinguistic models have been built for diagnostic and treatment decision-making • It is possible that children with the same locus of impairment form clinical SSD subgroups
Technical Challenges • Factors to consider when attempting to assign a label to a case • Age of first assessment referral • Error pattern at first assessment • Speech sound accuracy across various structural levels, e.g., single words vs. conversation • Treatment approach • Two children may work on the same speech sound at age 8 • One was just referred for the first time and never had any other sounds in error • One was diagnosed with CAS at age 4 and had intense treatment since then • It follows that a child’s speech error profile can change dynamically across time
Appraising Current SSD Nosologies Multiple ways of classifying speech sound disorders co-exist Which has the best statistical validity? Which has the best clinical validity? How can we arrive at a universally accepted classification?
New Frontiers: Empirical Classification • Rather than creating theory-derived categories and labels, let’s have the children classify themselves! • Idea: data-based clustering • Recipe: • Many children with whatever speech problems they may have • Each child is tested with many different types of tests of speech ability (phoneme inventory, phonological processes, intelligibility) and other relevant areas (language, reading, motor, etc.) – all measures adjusted for age and sex • Hierarchical agglomerative clustering will show approximately how many clusters are present • K-means clustering will create clusters with highly similar cases and highly dissimilar clusters
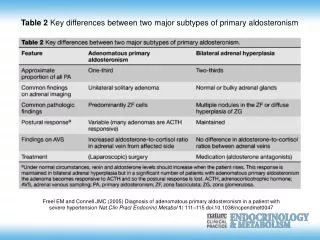
Cluster analysis in a multivariate dataset (Dodd, B. [2005]. Differential diagnosis and treatment of children with speech disorder (2nd ed.). London ; Philadelphia: Whurr) • 100 children, ages 3;0 to 5;6 • Six areas of motor functioning, represented by 18 different variables • Four clusters: • Deviant inconsistent errors • Deficits in oromotor and motor speech tasks • Articulatory groping, consonant deletion, differences between voluntary and involuntary movements • Prosodic errors and history of no babbling
Clustering in 12 preschool children with speech sound disorder and 12 age- and gender-matched controls (Peter, 2006) • Measures • Speech (articulation test, test of phonological processes) • Language (receptive vocabulary, sentence comprehension, sentence imitation) • Timing accuracy (vowel durations in a nonword repetition task, timing accuracy in a clapped rhythm task and a finger tapping task) • Three clusters in the children with speech sound disorder: • Overall high performance • Overall intermediate performance • Overall extremely poor performance, language scores in clinical range
Legend: A = lower articulation test score than phonology test score P = lower phonology test score than articulation test score C = at least 8 of 11 CAS traits regardless of other scores Peter, B. (2006). Multivariate characteristics and data-based disorder classification in children with speech disorders of unknown origin: WorldCat Dissertations and Theses.
New Frontiers: Biological Classification • Speech sound disorders run in families • Twin, adoption, and aggregation studies show that there is a genetic etiology • Caveat: • Genes plus environmental factors influence speech development! • Risk genotypes can have low penetrance! • Variations in the FOXP2 gene cause syndromic speech problems • A causal gene for nonsyndromic speech problems has not yet been identified
Molecular studies have looked at candidate regions in the genome in large groups of children with speech sound disorders and their siblings. • Traditional assumption • “Complex trait” • “Common disease/common variant”
Alternate view • “Common disease/rare variant” • “Mendelian” inheritance • In a given family, very few gene variants may be causal • Different variants in different families • Examples: autism, hearing impairment • Consistent with the new framework: • In a study of five multigenerational families with speech sound disorder, two families showed difficulties with alternating movements, compared to repetitive movements (oral, hand) (Peter & Raskind, 2011) • Genome-wide genetic linkage analysis in one of these families showed four new regions of interest (Peter, Matushita & Raskind, in press), one that overlapped with a candidate region in dyslexia on chromosome 6 (Konig et al., 2010). The linked trait in the dyslexia study was rapid naming with alternating stimuli (colors and objects)
What can be gained in the long run by genetic studies? • Subtypes defined by biological etiology • More accurate diagnosis • Underlying deficits (e.g., sequencing) can be identified and treated • Early identification of at-risk status • New research in early intervention strategies in at-risk infants • New studies of biochemical pathways, gene expression, and – who knows? – pharmacogenetic approaches. • What are the dangers of genetic studies? • Insurability: Less problematic, thanks to the Genetic Information Nondiscrimination Act (GINA) of 2008 • Privacy: DNA sequences may be shared on online repositories, but there are excellent safeguards in place and data are only shared anonymously.
Connections Chapter 1: Theoretical considerations Chapter 2: Tools for identifying strengths and weaknesses across a variety of tasks Chapter 18: Motor speech disorders Chapter 20: Assembling these tools for purposes of assessment and diagnosis Chapter 21: Various treatment approaches that were designed for certain types of children with SSD Williams, McLeod & McCauley (2010) list many treatment approaches by approach category and describe target populations for each approach
Concluding Remarks A universally accepted SSD nosology does not yet exist Much work lies ahead in identifying SSD subtypes with clinical and statistical relevance Progress toward this goal will inform us in helping individuals with SSD overcome their communication barriers
Sidebar 15.1 “Lissa” Lissa(the names of all children in this chapters were changed to protect their privacy) was a bright sixth-grader whose speech was characterized by vowelization and [w] substitutions of /r/. No other speech sounds were in error. Several of her classroom teachers had referred Lissa for speech evaluations in the past starting in third grade, but her parents had resisted the idea of their gifted daughter receiving speech therapy. Lissa was keenly aware of her inability to produce /r/ and the difference between her speech production and that of her peers. At the beginning of sixth grade, she told her parents that she felt self-conscious and really wanted help for her speech. The parents finally agreed to the evaluation and also to the recommended course of treatment, and Lissa began to see the speech-language pathologist at her school for twice-weekly individual sessions. It took several sessions before Lissa was able to produce her first [r] in isolation. Despite Lissa’s good cooperation, her progress was slow and her productions of [r] were variable.
Sidebar 15.2 “Kyle” Kyle was a first-grader whose parents sought professional help from a private speech-language pathologist service because of concerns regarding his speech. Kyle’s speech was characterized by a frontal lisp ([ð] for /z/ and [θ] for /s/). He also substituted [f] for /θ/. In a way, the phonemes in his relational inventory were playing musical chairs: /s, z/ were missing from his sound inventory altogether. Where an /s/ was the target, he produced [θ], and where the /θ/ was the target, he produced [f] instead. Kyle’s parents were not only aware of his speech production errors but also began to notice that he spelled the way he talked (“teef” for teeth and “thun” for sun). Using a mouth model and a mirror, the clinician showed Kyle the articulatory positions for alveolar, interdental, and labiodental sounds. Kyle learned to sort word cards into bins representing each of these places of articulation. The word cards were created using minimal pairs such as “free” and “three,” “sink” and “think,” and “sound” and “found.” Next, Kyle worked on producing /s, z/, the sounds missing from his inventory, in isolation, syllables, words, and sentences. Using minimal pairs as stimuli, Kyle worked toward eliminating the [f] for /θ/ substitution. In the process of reorganizing his sound inventory, he went through a brief phase of overgeneralization, where he substituted [s] for /θ/. His diligence and his parents’ support payed off and he was dismissed from treatment after only four months when all of his target sounds were produced correctly in conversation.
Sidebar 15.3 “Mia” Mia was a lively Kindergartener who watched the news along with her parents at night and could cogently converse about current political events. While her teacher was very impressed with her precocious intellect, she had concerns about her speech as she consistently substituted [t] for /k/, [d] for /g/, and [n] for /ŋ/. Mia was referred for an evaluation and began twice-weekly sessions with the school’s speech-language pathologist. Following perceptual accuracy checks and an introduction to places of articulation using a mouth model as a visual aid, Mia attempted production of /k/ in isolation. She was exuberant when she heard herself produce the sound for the first time. Within two months of treatment, all velars had generalized into conversational speech and Mia was exited from treatment.
Sidebar 15.4 “Tom” As soon as Tom reached his third birthday, his parents referred him for a speech evaluation in the public school district where they lived. They had been concerned about this speech since he was a toddler and they had already obtained a hearing test to rule out hearing loss as a cause. At the time of the evaluation, Tom’s parents said that they had difficulty understanding him and frequently asked Tom to confirm whether their guess was correct. Over time, Tom had developed signs of extreme frustration and sometimes acted out or, worse, sometimes gave up trying to talk when he was not understood. Articulation testing and conversational samples showed that Sam’s speech was characterized by a frontal lisp, various sound substitutions ([ð] for /j/, [w] for /j/, [w] for /r/, [f] for /θ/), sound omissions ([nopaʊ] for “snowplough”), syllable omissions ([bun] for “balloon”), vowel errors ([to] for “toy”), sequencing errors ([ʃawaf] for “shovel”), and inconsistent productions of the same word ([pεðεn, pεnε] for “present”). Tom began to meet with the speech-language pathologist twice per week. His course of treatment was custom-made for him and consisted of elements of various approaches. Tom made rapid progress. By the time he started kindergarten, the only residual speech errors were the frontal lisp and the substitution of [f] for /θ/, and he now eagerly communicated his ideas without any signs of frustration or resignation. His case is discussed in more detail in a published book chapter: Peter, B. (2010a). Complex disorder traits in a three-year-old boy with a severe speech-sound disorder. In S. Chabon & E. Cohn (Eds.), Communication disorders: A case-based approach. Delaware: Pearson.
Sidebar 15.5 “Jenna” Jenna was 5;1 when her teacher referred her for a speech assessment. During standardized articulation testing, which involved single-word productions in response to a picture stimulus, the following sound distortions, substitutions, and omissions were noted: • θ/s. ð/z (frontal lisp) • ʃl, ʧl, ʤl (lateralized airflow on palatal fricatives and affricates) • t/k, d/ɡ, n/ŋ (velar fronting) • d/ɡr, t/kl, θ/sp (cluster reduction) • bənunθ/bəlunz (assimilation and final devoicing) • wɪn/rɪŋ, faʊɜθ/flaʊɚz (gliding and derhotacization) • a:f/naɪf (initial consonant deletion and vowel error) • bæt/bæθ (stopping) • j/ð, v/b, nəʤlæmən/pəʤæməz (unusual and idiosyncratic errors) The fact that Jenna had so many errored speech sounds and patterns, together with concerns about her ability to make herself understood in school and at home, were taken into consideration when the decision was made to qualify her for treatment.
Sidebar 15.6 The “Collins” Family Trevor was a second grader who saw the school’s speech-language pathologist for twice weekly sessions to address multiple speech errors including a frontal lisp and liquid substitutions. His older sister, a fourth grader, had received speech therapy for similar sound errors and was close to being dismissed from treatment. Two younger children in the family, ages 5 and 3 years, had been assessed and qualified for speech services because of multiple speech sounds in error. The children’s mother spoke with a frontal lisp and reported that both she and her brother had had a childhood history of disordered speech; only her brother, however, had received speech services. The speech-language pathologist wrote a family treatment plan in which she outlined some general concepts regarding speech sound production as well as principles of treatment and some suggested activities and materials. This document was helpful in supporting home practice for the children, and the children’s mother reported that she herself took a more active role in her children’s home speech assignments, which helped her to become more aware of her own distorted speech sounds and to increase correct productions in her own speech.