Download
1 / 29
290 likes | 439 Views
Proteomic Profiling by Antibody Micro-Array. Kent J. Johnson M.D. Roscoe L. Warner Ph.D. Piezorray Non-Contact Printer. Micro-Array System. Y Y. Y Y. Y. Y. Y. DyLight 650 NeutrAvidin. Y. Y Y. Y. Y Y. Y. Y. Y. Biotinyled Secondary Antibody. Y. Y Y. Y. Y. Sandwich ELISA.

E N D
Proteomic Profiling by Antibody Micro-Array Kent J. Johnson M.D. Roscoe L. Warner Ph.D.
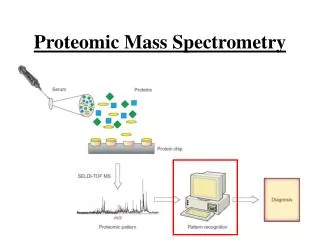
Micro-Array System Y Y Y Y Y Y Y DyLight 650NeutrAvidin Y Y Y Y Y Y Y Y Y Biotinyled Secondary Antibody Y Y Y Y Y Sandwich ELISA Target Antigens (Std. or Sample) Y Y Y Y Y Y Y Y Y Y Primary Antibodies MFI Intensity of Standards Used for Calculation of Unknowns
Representative Well Chip Primary Antibodies ….. ….. ….. ….. ….. ….. ….. ….. ….. ….. ….. ….. ….. ….. ….. ….. ….. ….. ….. ….. IL-2 IL-6 IL-8 IL-10 IL-17 IL-2R TNFa IFNg GM-CSF IP-10 RANTES EGF MCP-1 MCP-3 MMP-7 KIM-1 Isotype Controls: Mouse, Rabbit, Human Each spot receives 325 picoL of antibody solution applied to Sialylated Chips as a Piezorray-static spray Spot size: 120 mm
Chip-Plate Technology using 5 chips in an 80 well grouping Prototype Lab (UM: Medical Innovation Center)
Chip-1 Chip-2 Chip-3 Chip-4 Chip-5 Standard Curve
Cross-Reactivity Testing Second Series First Series DyLight 550 NeutrAvidin DyLight 650 NeutrAvidin Y Y Y Biotinylated Secondary Antibody Y Y Y Y Y Y Biotinylated Secondary Antibody Y Specific Antigen YYYYY YYYYY YYYYY YYYYY YYYYY YYYYY YYYYY YYYYY YYYYY YYYYY YYYYY YYYYY YYYYY YYYYY YYYYY YYYYY YYYYY YYYYY MFI Intensity of DyLight 550 and DyLight 650
A. B. C. Determinations 1 2 3 4 5 6 Specific Binding of Antigen 1 2 3 4 5 6 Non-Specific Binding of Secondary Antibody
Development of Standard Curve and Linear Range Standards used as Log4 dilution of master mix plus a zero value. Standard Curve generated for each antigen and equation of the line determined. Antigen concentration of samples calculated from equation of the line.
Performance of Micro-Array Methodology Human Micro-Array Chip System
Advantages of Custom Antibody Micro-Array • Easily modified to accommodate unique target antigens. • Ability to custom develop chips for desired species, limited • only by availability of purified antigen and antibodies. • 3. Quantifiable approach to high throughput analysis of multiple • antigens using small sample size. • 4. Only One U.S. company to date makes Antibody Arrays. • 5. Comparable technologies include ELISA, Bead-based assays,
Rat Models Dermal Arthus Glucan Streptozotocin Induced Diabetes Gentamicin Cyclosporin A Fenoldopam
Cyclosporin A Injury *Significantly Different (p < 0.05), Mean +/- SD of Cyclosporin treated rats (n=10) and normal healthy (n=10) control animals.
Analytes of Wegener’s Granulomatosis Patients . Proteins Normal (pg/mL) Wegener’s Fold Granulomatosis change (pg/mL) . ACE-1 3,290.1 (+/- 214.3) 5,927.1 (+/- 283.0)* + 1.8 IFN-g 23.4 (+/- 3.4) 151.4 (+/- 19.5)* + 6.5 IL-8 1.7.3 (+/- 9.0) 1,294.0 (+/- 55.3)* + 12.1 s-ICAM 6,195.2 (+/- 533.7) 12,679.4 (+/- 870.7)* + 2 s-VCAM 120.7 (+/- 26.5) 674.3 (+/- 28.8)* + 5.6 . The quantified values along with standard error of the mean (in parenthesis) are shown and allow for comparison of normal (n=30) and WG serum (n=26) samples. The fold change shows the difference between the normal and affected patients with positive (+) indicating an increase in WG patient serum.
RAVE Clinical Trial Rituximab in ANCA-Associated Vasculitis (RAVE) trial Long-term program to identify markers that are clinically useful in staging vasculitis activity, distinguishing vasculitis from other inflammatory diseases such as infections, and predicting response to treatment and risk of relapse.
Of the 186 subjects evaluated at screening, 139 had been diagnosed with GPA and 46 with MPA; 124 were positive for anti-PR3 and 62 for anti-MPO 93 had active glomerulonephritis 90 had a new diagnosis of AAV 96 had established diagnoses and were experiencing relapses. At screening: 92 patients were receiving glucocorticoids, and 104 were receiving some immune-suppressive drug (glucocorticoids, other drugs, or both). The 68 healthy controls included 28 males and 40 females, median age 41.
Use of Multiple Markers to Better Distinguish Severe or Mild Vasculitis from Remission Four markers (CXCL13/BCA-1, G-CSF, IL-15, and TIMP-1) were significantly higher at month 6, after adjustment for multiple comparisons, in the 25 subjects with active disease than in the 137 subjects in remission, Five additional markers (IFNg, CXCL8/IL-8, sIL-2R, CCL5/RANTES) might be higher based on unadjusted P values of < 0.05. Discrimination between mild disease and remission at month 6 was limited, with all AUC < 0.7
Based on logistic regression models with active disease vs. remission as the dichotomous outcome, the set of markers that best distinguished active AAV from remission in the 137 subjects with paired samples was: ACE (negatively), GM-CSF, MMP-3, TIMP-1, and ESR, with AUC=0.96. Odds ratios (for active AAV vs. remission in these 137 subjects) associated with 2-fold changes in these markers. When these 5 markers were used to model data limited to month 6, comparing 25 subjects with milder active AAV to 137 in remission, AUC=0.78.
Biomarkers In Patients with Biopsy Proven Rejection of Renal Allografts
Our findings demonstrate that the protein signature of healthy subjects is distinctly different from renal transplant patients with good allograft function and no previous history of rejection. We have identified 10 proteins that can reliably differentiate stable renal transplant recipients from healthy subjects in both the training and validation cohorts. Cystatin-C, EGF, GM-CSF, IL-1 R1, IL-5, KIM-1, MCP-1, MCP-3, MIF, TIMP-4 In addition, 17 proteins were identified that can differentiate rejecting renal transplant recipients from stable renal transplant patients. TGF-β2, E-Cadherin, GROα, TGF-β1, IL-6, IL-1 R1, EGF, MIP-3α, TNF-RII, KIM-1, Osteopontin, VEGF-R2, Epo-R, MIF, IL-12p70, MCP-1, GM-CSF The ultimate goal of the protein array is be to monitor non-invasively, renal transplant patients over time in order to detect subclinical changes before they would be detected by conventional methods, ie., change in serum creatinine levels, with the intent to alter long-term graft outcome.