Download
1 / 1
10 likes | 147 Views
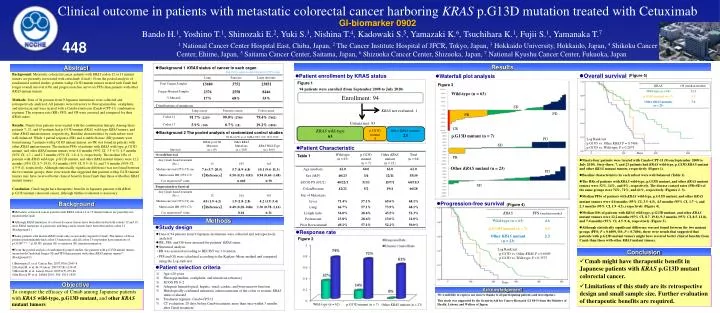
Clinical outcome in patients with metastatic colorectal cancer harboring KRAS p.G13D mutation treated with Cetuximab GI-biomarker 0902. Enrollment: 94. SD. PD. PR.

E N D
Clinical outcome in patients with metastatic colorectal cancer harboring KRAS p.G13D mutationtreated with Cetuximab GI-biomarker 0902 Enrollment: 94 SD PD PR Bando H.1, Yoshino T.1, Shinozaki E.2, Yuki S.3, Nishina T.4, Kadowaki S.5, Yamazaki K.6, Tsuchihara K.1, Fujii S.1, Yamanaka T.7 448 1 National Cancer Center Hospital East, Chiba, Japan, 2 The Cancer Institute Hospital of JFCR, Tokyo, Japan, 3 Hokkaido University, Hokkaido, Japan, 4 Shikoku Cancer Center, Ehime, Japan, 5 Saitama Cancer Center, Saitama, Japan, 6 Shizuoka Cancer Center, Shizuoka, Japan, 7 National Kyushu Cancer Center, Fukuoka, Japan CR KRAS wild-type 63 p.G13D mutant 7 Other KRAS mutants 23 Results Abstract • Background 1 KRAS status of cancer in each organ • http://www.sanger.ac.uk/perl/genetics/CGP/cosmic Background: Metastatic colorectal cancer patients with KRAS codon 12 or 13 mutant tumors are presently not treated with cetuximab (Cmab). From the pooled analysisof randomized control studies, patients with p.G13D mutant tumors treated with Cmab had longer overall survival (OS) and progression-free survival (PFS) than patients with other KRAS mutant tumors. Methods: Data of 94 patients from 9 Japanese institutions were collected and retrospectively analyzed. All patients were refractory to fluoropyrimidine, oxaliplatin, and irinotecan and were treated with a Cmab+irinotecan (Cmab+CPT-11)combination regimen. The response rate (RR), PFS, and OS were assessed and compared for their KRAS status. Results: Ninety-four patients were treated with the combination therapy. Among these patients 7, 23, and 63 patients had p.G13D mutant KRAS, wild-type KRAS tumors, and other KRAS mutant tumors, respectively. Baseline characteristics by each subset were well-balanced. While 1 partial response (PR) and 4 stable disease (SD) patients were found among 7 patients with p.G13D mutant tumors, no PR was found in patients with other KRAS mutant tumors. The median PFSs of patients with KRAS wild-type, p.G13D mutant, and other KRAS mutant tumors were 4.6 months (95% CI, 3.5–6.5), 4.5 months (95% CI, 1.7-), and 2.3 months (95% CI, 1.9–4.3), respectively. The median OSs of patients with KRAS wild-type, p.G13D mutant, and other KRAS mutant tumors were 12.2 months (95% CI, 8.7–19.8), 9.3 months (95% CI, 8.5–11.8), and 7.4 months (95% CI, 4.5–9.4), respectively. Although statistically significant difference was not found between the two mutant groups, there were trends that suggested that patients with p.G13D mutant tumors may have received better clinical benefits from Cmab than those with other KRAS mutant tumors. Conclusion: Cmab might have therapeutic benefits in Japanese patients with KRAS p.G13D mutant colorectal cancer, although further evaluation is necessary. • Overall survival • Patient enrollment by KRAS status (Figure 5) • Waterfall plot analysis Figure 1 Figure 3 94 patients were enrolled (from September 2008 to July 2010) Wild-type (n = 63) KRAS not evaluated: 1 Distributions of mutations Criteria met: 93 • Background 2 The pooled analysisof randomized control studies p.G13D mutant (n = 7) De Roock W, et al. JAMA 2010; 304: 1812-1820. PD Log Rank test p.G13D vs. Other KRASP = 0.7406 p.G13D vs. Wild-type P = 0.2075 SD • Patient Characteristic Days Table 1 PR • Ninety-four patients were treated with Cmab+CPT-11 (From September 2008 to July 2010). Sixty-three, 7, and 23 patients had KRAS wild-type, p.G13D KRAS mutant and other KRAS mutant tumors, respectively (Figure 1). • Baseline characteristics by each subset were well-balanced (Table 1). • The RRs of patients with KRAS wild-type, p.G13D mutant, and other KRAS mutant tumors were 32%, 14%,and 0%, respectively. The disease control rates (PR+SD) of the same groups were 74%, 71%, and 61%, respectively (Figures 2–3). • Median PFSs of patients with KRAS wild-type, p.G13D mutant,andother KRAS mutant tumors were 4.6 months (95% CI, 3.5–6.5), 4.5 months (95% CI, 1.7–), and 2.3 months (95% CI, 1.9–4.3), respectively (Figure 4). • Median OSs of patients with KRAS wild-type, p.G13D mutant,and other KRAS mutant tumors were 12.2 months (95% CI, 8.7–19.8), 9.3 months (95% CI, 8.5–11.8), and 7.4 months (95% CI, 4.5–9.4), respectively (Figure 5). • Although statistically significant difference was not found between the two mutant groups (PFS; P = 0.6009, OS; P = 0.7406), there were trends that suggested that patients with p.G13D mutant tumors might have received better clinical benefits from Cmab than those with other KRAS mutant tumors. Other KRAS mutant (n = 23) PD SD Background • Progression-free survival (Figure 4) • Metastatic colorectal cancer patients with KRAS codon 12 or 13 mutant tumors are presently not treated with Cmab. • Although KRAS mutations of colorectal cancer tissues have been detected in both codons 12 and 13, most KRAS mutations of pancreatic and lung cancer tissues have been detected in codon 12 (Background 1). • Some patients with mutant KRAS status only occasionally respond to Cmab. The tumors of those patients predominantly had codon 13 mutations, and all codon 13 responders have mutations of p.G13D*1)-3). * p.G13D: glycine (G) to aspartate (D) transition mutation • From the pooled analysisof randomized control studies, the patients with p.G13D mutant tumors treated with Cmab had longer OS and PFS than patients with other KRAS mutant tumors4) (Background 2). • Benvenuti S, et al. Cancer Res. 2007,67(6):2643-8. • Frattini M, et al. Br J Cancer. 2007;97(8):1139-45. • Moroni M, et al. Lancet Oncol. 2005;6(5):279-86. • De Roock W, et al. JAMA 2010; 304: 1812-1820. Methods • Study design • Response rate • Data of 94 patients from 9 Japanese institutions were collected and retrospectively analyzed. • RR, PFS, and OS were assessed for patients’ KRAS status. • Statistical analysis • ・RR was assessed according to RECIST ver.1.0 criteria. • ・PFS and OS were calculated according to the Kaplan–Meier method and compared using the Log-rank test. Figure 2 Log Rank test p.G13D vs. Other KRASP = 0.6009 p.G13D vs. Wild-type P = 0.3575 Conclusion • Cmab might have therapeutic benefit in Japanese patients with KRAS p.G13D mutant colorectal cancer. • Limitations of this study are its retrospective design and small sample size. Further evaluation of therapeutic benefits are required. • Patient selection criteria • Age >20 years • Fluoropyrimidine, oxaliplatin, and irinotecan refractory • ECOG PS 0–2 • Adequate hematological, hepatic, renal, cardiac, and bone marrow function • Histologically confirmed metastatic adenocarcinoma of the colon or rectum; KRAS status evaluated • Treatment regimen: Cmab+CPT-11 • CT evaluation: 28 days before Cmab treatment, more than once within 3 months after Cmab treatment Days Objective Acknowledgement To compare the efficacy of Cmab among Japanese patients with KRAS wild-type, p.G13D mutant, and other KRAS mutant tumors We would like to express our sincere thanks to all participating patients and investigators. This study was supported by the Grant-in-Aid for Cancer Research (21 S4-5) from the Ministry of Health, Labour, and Welfare of Japan. Wild-type (n = 62) p.G13D mutant (n = 7) Other KRAS mutant (n = 23)