Download
1 / 82
820 likes | 832 Views
Learn about the basics of diabetes, insulin production, glucose regulation, and the role of nursing in providing good diabetes care. Understand the different types of diabetes and their treatment options.

E N D
USA’s Growing Population with Diabetes Millions of People Data from the National Diabetes Statistics Report, 2014 (released June 10, 2014) - See more at: http://www.diabetes.org/diabetes-basics/statistics/#sthash.dC2iwT48.dpuf
Why Nursing is Vital & Well-Positioned to Help Provide Good Diabetes Care • Nursing sees the whole picture & plays many roles in patient care • e.g, travel off unit, physical therapy, X-ray • Amount of food eaten (carbs) or NPO status • Patient’s day to day concerns • Order changes (by various providers) • Observer of changes in symptoms • Nursing does most (if not all) of the patient education
Diabetes in the Acute Care Setting • Basics – Review of Pathophysiology • Prevention/Treatment • Lifestyle Modifications • Insulin & Oral Agents • Hypo/Hyperglycemia Review • The Complications • Inpatient Diabetes Care/Patient Education • Case Studies
BasicsEnergy Balance – Insulin Production It All Starts with the Eyes & Nose Anyone Hungry???
BasicsEnergy Balance – Insulin Production Bloom S et al. Hormonal regulation of food intake. Physiol Rev 2005;85(4):1131-58.
BasicsInsulin Uptake into the Cells Harvard Health Publications
Basics-The Body’s Response to Efficient Circulating Insulin Hyperglycemia Adiposetissue Liver Muscle Glucoseuptake Stored as fat Glucose storage Glucose uptake for energy Euglycemia
Basics-The Body’s Response to Little or No Circulating Insulin Hyperglycemia Liver Muscle Defective Glucose storage Defective Glucose uptake for energy Defective Glucoseuptake ↑ ↑ ↑Hyperglycemia
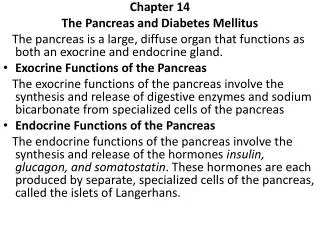
BasicsDefinition of Diabetes Mellitus Diabetes mellitus is a group of metabolic diseases characterized by hyperglycemia resulting from defects in insulin secretion, insulin action, or both. The chronic hyperglycemia of diabetes is associated with long-term damage, dysfunction, and failure of various organs, especially the eyes, kidneys, nerves, heart, and blood vessels.
Basics – The Numbers & Targets • Normal fasting glucose FPG <100 mg/dl (5.6 mmol/l) • Impaired fasting glucose (IFG) or “Pre-Diabetes” FPG 100–125 mg/dl (5.6–6.9 mmol/l) or A1c 5.7-6.4% • Diabetes (with A1c or OGTT) FPG ≥126 mg/dl (7.0 mmol/l) or A1c >6.5% • Targets*: • Critical Care 140-180 mg/dL • Non-critical care pre-meal <140 mg/dL • Non-critical care random <180 mg/dL • Outpatient: A1c <7%; 80-130 mg/dL for most patients; individualize to patient health state *ADA Standards of Medical Care in Diabetes – 2015
Basics – Glycated Hemoglobin or HbA1c An HbA1c or “A1c” test is the measure of the average blood glucose over the past 2-3 months. When BG are high, glucose molecules attach to the hemoglobin in RBCs. The longer hyperglycemia occurs, the more glucose binds to the RBC & the higher the A1c.
Basics – Type 1 Diabetes (T1DM) • Characterized by labile glycemic control; sensitivity to both insulin & glucose • Associated with microvascular and macrovascular complications • Generally arises from an autoimmune process that destroys the pancreatic β-cells • Reduced or absent glucagon release
Basics – T1DM Treatment Before/After Discovery of Insulin Elizabeth Hughes, 1918 (left), age 11, during starvation therapy. Elizabeth Hughes, 1921 (right) age 14 after start of insulin therapy. She lived until 1981; outlived her T1DM life expectancy by 60 years.
Basics – What is Insulin Sensitivity? • Insulin sensitivity is a term used to describe people who require relatively normal or low levels of insulin to process glucose. • A person who is insulin-sensitive needs only a relatively small amount of insulin to keep blood glucose levels in the normal range and to keep the body’s cells supplied with the glucose they need. • T1DM & s/p total pancreatectomy patients are usually insulin sensitive
Basics – Type 2 Diabetes (T2DM) • Characterized by chronic hyperglycemia; insulin resistance • Associated with microvascular and macrovascular complications • Generally arises from a combination of defective insulin uptake and -cell dysfunction
IR Basics – What is Insulin Resistance? • Opposite of insulin sensitive, an insulin resistant patient needs much more insulin to achieve the same BG lowering effects. • Major defect in individuals with T2DM • Reduced biological response to insulin (will require larger doses of insulin than T1DM) • Strong predictor of T2DM • Closely associated with obesity, especially visceral adiposity
IR Basics – Insulin Resistance Reduced Response to Circulating Insulin Insulin resistance Adiposetissue Liver Muscle Glucoseuptake Glucose uptake Glucoseoutput Hyperglycemia
Basics – What is -cell dysfunction? • Major defect in individuals with type 2 diabetes (inherited) • Reduced ability of -cells to secrete insulin in response to hyperglycemia over time
Prevention/TreatmentChanging Behaviors • Healthy Eating • Activity • Healthy Coping/Stress Management R E L A P S E The Transtheoretical Model (Prochaska & DiClemente, 1983)
Prevention/Treatment – Healthy Eating • Moderate intake of carbohydrates (26-45% of daily calories come from carbohydrates) • Men 3-4 servings or 45-60 grams per meal • Women 2-3 servings or 30-45 grams per meal • *Very low carb diets not endorsed (20-50g/day) • Increase consumption of vegetables and fruits and low dairy products (DASH diet) • Reduce saturated fat, cholesterol and trans fat intake (but not fat free) • Reduce sodium intake • Moderate intake of alcohol ADA, 2015
Prevention/Treatment – Activity • Children with diabetes or prediabetes – 60 minutes of physical activity daily • Adults with diabetes or prediabetes – 150 min/week of moderate-intensity aerobic physical ativity (50-70 of maximum heart rate) spread over at least 3 days/week with no more than 2 consecutive days without exercise • Adults with T2DM – twice weekly resistance training
Prevention/Treatment – Activity • Evidence supports that ALL individuals, diabetes or not, should reduce sedentary time, break up extended time (>90 min.) spent sitting ADA, 2015
Prevention/Treatment – Healthy Coping Short term stress response Long-term stress response Effects of glucocorticoids/ cortisol: Proteins and fats broken down into glucose, leading to increase blood glucose Effects of mineralocorticoids: Retention of sodium ions & water by the kidney Increased blood volume & pressure Impact of counter-regulatory hormones: epinephrine & noepinephrine • Glycogen broken down into glucose, raising blood glucose • Increased blood pressure • Increased breathing rate • Increased metabolic rate • Chang in blood flow patterns, leading to increased alertness, decreased digestion & renal activity
Prevention/Treatment – Healthy Coping • Recognize stress, know your triggers and understand it can be managed. • Learning/Practicing healthy techniques that help you cope. (quiet time, exercise, music, reading, talking with supportive friend)
Prevention/Treatment – Healthy Coping • Setting realistic expectations & promoting healthy coping behaviors • Setting realistic goals (think what we sometimes as our patients to do) • Reasonable schedules • Regular exercise • Appropriate assertiveness • Eating Healthy • Getting enough sleep • Avoiding unhealthy behaviors • Breathe…. Frydenberg, E.Thriving, Surviving, or Going Under: Coping with Everyday Lives, Information Age, 2004
IR How to combat insulin resistance? • Loss of body fat • Exercise • Good blood glucose control • Stress management • Adequate sleep • Food choices-moderation, reduced carbohydrate intake
Insulin response to blood glucose levels (no Diabetes) 180mg/dL Blood Glucose Levels 99mg/dL Insulin Effect 70mg/dL Lunch Breakfast Dinner Body releases insulin in response to actual glucose levels Body releases a small amount of insulin 24/7 to keep blood glucose stabilized.
Basal-Nutritional Therapy-mimicking the body’s natural insulin response- 180mg/dL Blood Glucose Levels Insulin Effect 99mg/dL 70mg/dL Lunch Breakfast Dinner Rapid Acting Insulin (i.e. lispro-Humalog) Long Acting Insulin (i.e. glargine-Lantus)
3 Reasons to Administer Insulin for BG ControlAlways Ask Yourself “Why Am I Giving this Dose of Insulin”? • Basal-long acting to suppress gluconeogenesis between meals or at night • Nutritional/Bolus-rapid/fast acting to cover intake of carbs (e.g. meals, Tube Feeds) & prevent post-prandial/meal hyperglycemia • Correction (sliding scale)-rapid/fast acting insulin to cover existing hyperglycemia
Insulin on Board • “Insulin on Board” simply refers to the amount of insulin still circulating in the bloodstream that may still be working. • Be mindful of what patient has already received & how long it is acting • Prevent Over-Reaction-watch BG trends! I I
Insulin Stacking • Remember “Insulin on Board” • Stacking insulin refers to when a patient receives more insulin before the previous amount of insulin given has finished working. This creates even more onboard insulin. • When insulin stacking can lead to serious episodes of hypoglycemia.
Insulin Pump Therapy Insertion Set – holds delivery canula in place in the subcutaneous tissue Insulin Pump – preprogrammed technology that holds all basal, nutritional and correction coverage settings. Basal insulin delivered around the clock. Nutritional and correction boluses manually entered dependent on carbohydrate intake and blood glucose levels.
Continuous Glucose Monitoringaka “Sensor” Sensor – held in place in the subcutaneous tissue Receiver – blood glucose levels wirelessly transmitted to receiver to give user blood glucose trends. CGM & insulin pump technology combined.
Oral Agents *Watch for hypoglycemia especially if patient not eating/NPO Sutter Health. Diabetes Handbook, 2014
Oral Agents Sutter Health. Diabetes Handbook, 2014
Oral Antidiabetic Meds in Hospitalized Patients • Most oral agents are optimized in outpatient settings. • If a patient is NPO or eating very little in the wake of illness, oral agents may cause hypoglycemia. • However, the stress of most illnesses can cause insulin resistance & worsen control with agents alone. • Contrast dye: 48 hour post test hold of metformin • Renal Failure: Contraindicated for metformin & SFU (e.g. glyburide) • Where do we go from outpatient oral agents to inpatient insulin... Start with a Correction Scale!
Other Injectables Sutter Health. Diabetes Handbook, 2014
Diabetes Treatment Pitfalls in the Hospital • Home medication plan dc’d & pt put on insulin scale only • Pt not on CHO controlled diet • RNs/NAs not accurately watching pt nutrition intake for pts on insulin or oral meds therapy • MDs not changing insulin plans when hyper/hypoglycemic • Large doses of long acting insulin given then pt made NPO (“overbasalization”) or TF stopped with large dose on board • Pt hypoglycemia over treated resulting in rebound hyperglycemia