Download
1 / 62
620 likes | 657 Views
Learn about lymphoid neoplasms, their impact on the immune system, diagnostic processes, etiology including genetic and environmental factors, and treatment options. Explore the WHO classification and origins of different types of lymphoid neoplasms.

E N D
Lymphoid Neoplasm Nirwansyah Parampasi Department of Pathology Untad
Neoplastic proliferations of white cells • Lymphoid Neoplasms • Myeloid Neoplasms - Acute myelogenous leukemia - Myelodysplastic syndromes - Chronic myeloproliferative disorders • Histiocytosis Langerhans cell hitiocytosis
Lymphoid Neoplasmsclose to immune regulatory system • Lymphoid neoplasm are tumors of the immune system disrupt normal immune regulatory mechanisms • Evidences: susceptibility to infection, autoimmune diseases
Lymphoid Neoplasmsclose to immune regulatory system • Patients with inherited or acquired immunodeficiency are at high risk of developing certain lymphoid neoplasm, particularly these associated with EBV infection
Lymphoid Neoplasms • All lymphoid neoplasms are derived from single transformed cell monoclonal • Divided into 2 big groups: - Non Hodgkins Lymphoma(NHL) - Hodgkins Lymphoma (HL)
Lymphoid Neoplasms • NHLs often present as involvement of a particular tissue site • Sensitive molecular assay usually show that the tumor is widely disseminated at the time of diagnosis only systemic therapy are curative
Lymphoid Neoplasms • HLs are often presents at a single site spreads methodically to contiguous lymph nodes group • Early course tumors may be cured with local therapy alone
Lymphoid Neoplasms • HL spreads in orderly fashion, and as a result STAGING is of importance in determining therapy • The spread of NHL is less predictable most patients are assumed to have systemic disease at the time of diagnosis staging in particular NHL provides useful prognosis information, but generally not important in guiding therapy
E T I O L O G Y • Chromosomal translocation: Chronic Meylocytic Lymphoma (CML), Burkitt lymphoma • Inherited genetic factors: Bloom syndrome, Fanconi anemia, ataxia telangiectasia, Down syndrome • Viruses: HTLV-1, EBV, KSHV, HHV-8 • Environmental agents: Helicobacter pylorii (gastric B-cell lymphoma), gluten-sensitive enteropathy (T-cell lymphoma), HIV (B-cell lymphoma) • Iatrogenic factors: radiotherapy & chemotherapy mutagenic effect
Lymphoid Neoplasms Certain relevant principles must be emphasized • Can be suspected from the clinical features, but histological examination of lymph nodes and other involved tissue is required for diagnosis • The vast majority of lymphoid neoplasm (80% - 85%) are of B-cell origin; most of the remainder being T-cell tumors; only rarely are tumors of NK origin encountered • Two basic forms of B-cell lymphoma: follicular & diffuse type
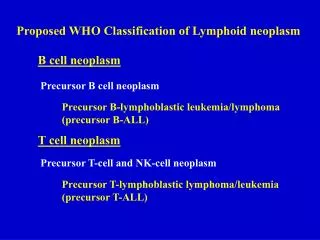
The WHO Classification of theLymphoid Neoplasms • Precursor B-cell Neoplasms: neoplasms of immature B-cells • Peripheral B-cell Neoplasms: neoplasms of mature B-cells • Precursor T-cell Neoplasms: neoplasms of immature T-cells • Peripheral T-cell and NK-cell Neoplasms: neoplasms of mature T-cell and NK-cell • Hodgkin Lymphoma: neoplasms of Reed-Sternberg cells and variants
Origin of Lymphoid Neoplasms CLP: common lymphoid precursor; BLB: pre-B lymphoblast; NBC: naive B-cell; MC: mantle B-cell; GC: germinal center B-cell; MZ: marginal zone B-cell; DN: CD4/CD8 double negative pre-T cell; DP: CD4/CD8 double positive pre-T cell; PTC: peripheral T-cell
Precursor B & T cell neoplasms • Acute lymphoblastic Leukemia (ALL): contain of immature cells, precursor B / T cells (lymphoblast) • 85% arising from precursor B cell childhood acute leukemia • The less common, from precursor T cell adolescent males lymphoma
Precursor B & T cells neoplasms • There is overlap in the clinical behaviour of B & T-ALL. • B-ALL uncommonly presents as a mass in the skin/ bone and T-ALL presents with leukemic picture • ALL must be distinguished from CML due to differing response to chemotherapy
The Classification of theLymphoid Neoplasms WHOPrecursor B-cell NeoplasmsDiagnosis: precursor B lymphoblastic leukemia/lymphoma • Asal: sel B prekursor sumsum tulang mengekspresikan TdT • tidakmengandung Ig permukaan • Genotipa: • translokasi kromosom t(12;21), • CBFα dan ETV6 rearrangement • Klinis:agresif • predominan pada anak-anak, • gejala : pansitopeni
The WHO Classification of theLymphoid NeoplasmsIII. Precursor T-cell NeoplasmsDiagnosis: precursor T lymphoblastic leukemia/lymphoma • Asal: prekursor sel T, sering dari timus • Mengekspresikan TdT • Genotipa: • Translokasi kromosom, lokus reseptor sel T • Paling sering rearrangement TAL1
Acute lymphoblastic leukemia / lymphoma • Originate from B-cell or T-cell, mostly from T-cell • Can be differed by B-cell marker CD22 • The nuclear chromatin is delicate and finely stippled, • and nucleoli are either absent or inconspicuous
The WHO Classification of theLymphoid NeoplasmsII. Peripheral B-cell Neoplasms • CLL / small lymphocytic lymphoma • B-cell prolymphocytic leukemia • Lymphoplasmacytic lymphoma • Splenic and nodal marginal zone lymphoma • Extranodal marginal zone lymphoma • Mantel cell lymphoma • Follicular lymphoma • Marginal zone lymphoma • Hairy cell leukemia • Plasmacytoma / plasma cell myeloma • Diffuse large B-cell lymphoma • Burkitt lymphoma
II. Peripheral B-cell Neoplasms Small Lymphocytic LeukemiaSmall Lymphocytic Lymphoma • The two indistinguishable disorders: - morphologically, phenotypically - genotypically differing in the degree of peripheral blood lymphocytosis • Proliferation center: loose aggregates of pro-lymphocyte pathognomonic • Tumor cells usually infiltrate the splenic white and red pulp, and the hepatic portal tract, although the extent of involvement varies widely.
II. Peripheral B-cell Neoplasms Small Lymphocytic LeukemiaSmall Lymphocytic Lymphoma Diffuse effacement of nodal architecture The majority of the tumor cells are small round lymphocytes. Arrow: pro-lymphocyte
II. Peripheral B-cell Neoplasms Follicular Lymphoma • The most common form of NHL in the USA (45% of adult lymphomas) • Usually present in the middle age and afflicts males and females equally • Less common in Europe, and rare in Asian population • The tumor cells closely resemble normal germinal center B-cells
II. Peripheral B-cell Neoplasms Follicular Lymphoma • In most cases, at low magnification, a predominantly nodular or nodular and diffuse growth pattern is observed • Involvement: bone marrow (85%), spleen, liver • Te overall median survival is 7 to 9 years, is not improved by aggressive therapy
II. Peripheral B-cell Neoplasms Follicular Lymphoma • Two principle cells are observed in varying proportion: (1) small cell with irregular or cleaved nuclear contour and scant cytoplasm centrocyte (2) larger cells with open nuclear chromatin, several nucleoli, and modest amount of cytoplasm centroblast
Follicular Lymphoma (spleen) Prominent nodules represent white pulp follicles expanded by follicular lymphoma cells
Follicular Lymphoma Malignant lymph follicles are marked by Bcl-2 positive
Follicular Lymphoma Small lymphoid cells with condensed chromatin and irregular or cleaved nuclear outline (centrocyte), mixed with a population of larger cells with nucleoli (centroblast)
Mantle cell lymphoma Neoplastic lymphoid cells surround a small, atrophic germinal center exhibiting mantle zone pattern of growth Homogenous population of small lymphoid cells with somewhat irregular nuclear outlines, condensed chromatin, and scant cytoplasm.
II. Peripheral B-cell Neoplasms Diffuse large B-cell lymphoma(DLBCL) • Slight male predominance • Average age about 60 years • 5% of childhood lymphoma • Clinically present with a rapidly enlarging, often asymptomatic mass, at a single nodal or extranodal site
Diffuse large B-cell lymphoma Spleen: typical isolated large mass
Diffuse large B-cell Lymphoma Tumor cells show prominent nucleoli
Diffuse large B-cell lymphoma Tumor cells with large nuclei, open chromatin, and prominent nucleoli
II. Peripheral B-cell Neoplasms Burkitt lymphoma • Categories: (1) African (endemic) Burkitt lymphoma, (2) sporadic (non-endemic), (3) a subset of aggressive lymphoma occuring in individual with HIV infection • Responds well to short-term, high dose chemotherapy (children & young adults) • Clinical feature Both endemic & non-endemic are found largely in children and young adults (30%) • Most tumor manifests at extra-nodal sites
Burkitt lymphoma Low power: many tingible body macrophages Starry sky appearance Monotonous appearance, tumor cells with multiple small nucleoli and high mitotic index (typical)
Burkitt Lymphoma Several starry sky macrophages was shown (arrows)
II. Peripheral B-cell Neoplasms Multiple myeloma of the skull The sharply punched-out bone lesions are most obvious in the calvarium
Multiple myeloma (bone aspirate) Normal marrow cells are replaced by plasma cells
Lymphoplasmacytic lymphoma Bone marrow biopsy: various degrees of plasma cell differentiation Mast cell
The WHO Classification of theLymphoid NeoplasmsIV. Peripheral T&NK-cell Neoplasms • T-cell prolymhocytic leukemia • Large granular lymhocytic leukemia • Mycosis fungoides / Sezary syndrome • Peripheral T-cell lymphoma, unspecified • Anaplastic large cell lymphoma • Angioimmunoblastic T-cell lymphoma • Enteropathy-associated T-cell lymphoma • Panniculitis-like T-cell lymphoma • Hepatosplenic γδ T-cell lymphoma • Adult T-cell leukemia/Lymphoma • NK/T-cell lymphoma, nasal type • NK-cell leukemia
IV. Peripheral T&NK-cell LymphomaPeripheral T-cell lymphoma • T-cell lymphoma without specific defining features fall collectively into the category of “unspecified” • Account for approximately half of all T-cell lymphoma in the western world • As a group they are aggressive malignant with low 5-yrs • They may be nodal or extra nodal • Variable expression most nodal expressing CD4+ • They may be associated with eosinophilia
IV. Peripheral T&NK-cell LymphomaPeripheral T-cell lymphoma A spectrum of small, intermediate, and large lymphoid cells, many with irregular nuclear contours.
IV. Peripheral T&NK-cell LymphomaAnaplastic large cell lymphoma mitosis
Anaplastic large cell lymphoma “Hallmark” cells with horseshoe-like or “embryo –like” nuclei and abundant cytoplasma lie near the center of the field. IHC: ALK protein
IV. The WHO Classification of theLymphoid NeoplasmsV. Hodgkin Lymphoma • Classical subtype Nodular sclerosis Mixed cellularity Lymphocyte-rich Lymphocyte depletion • Lymphocyte pre-dominance
V. Hodgkin Lymphoma:KLINIS • Manifes sebagai benjolan periferal, tidak sakit, mengenai satu atau lebih limfonodi • Penyebaran dapat diperkirakan (lewat saluran limfe aferen dan eferen) • Pada penyebaran lanjut makin sulit diprediksi karena mulai ada penyebaran hematogen • Simtom konstitusional (40%): demam ringan (kadang siklik), berkeringat malam, penurunan berat badan (10% dari bb), pruritus, sakit pada daerah tumor sesudah minum alkohol
V. Hodgkin Lymphoma:KLINIS • Karakteristik: defisiensi fungsi sel T • Disfungsi imunitas ini dapat diperberat dengan pemberian obat-obat imunosupresan • Pada 50% kasus ditemukan limfositopeni absolut • Imunitas humoral masih ada sampai akhir
Urut-urutan frekwensi lokasi • Cervical & mediastinal (anterior – nodular sclerosis type) • Axillar, inguinal, retroperitoneal • Antecubital, Popliteal, mesenterik
Lymphocyte predomi- Nant, (paling lembut). Umur <35th. L:P=4:1 V. Hodgkin Lymphoma Mixed cellularity, dekade 4-5. Cure rate 75% Lymphocyte rich Lymphocyte depleted. Paling agresif. Nodular sclerosis. Paling banyak, dengan prognosis baik. Cure rate 80-85%