Download
1 / 44
450 likes | 481 Views
Learn best practices for administration of ocular antibiotics to treat various eye infections effectively. Topical, subconjunctival, and systemic methods explained with emphasis on proper dosage and application.

E N D
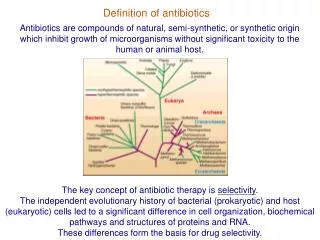
Administration of Ocular Antibiotics Antibiotics for eye infection can be given topically as drops or ointments, by subconjunctival or intravitreous injection, or systemically. Since the conjunctival sac can hold a volume of less than one drop, it is wasteful to instill more than one drop at a time.
When two different eye drops are required at the same time, dilution and overflow may occur when one immediately follows the other; an interval of 10-15 minutes should be allowed between the two applications.
It is important that the patient does not squeeze the eye shut after administration of the drop, as this will eliminate the fluid from the conjunctival sac. If necessary, the lid should be gently held open for 1 to 2 minutes after a drop has been administered.
Systemic absorption, which may occur after topical application of eye drops, can be minimized by using the finger to compress the lacrimalsac at the medial canthus for at least one minute after instillation of the drops. This helps block the passage of the drops through the nasolacrimal duct.
Eye ointments are applied similarly; the ointment melts rapidly and blinking helps to spread it. Eye ointments are retained for a longer period in the conjunctival sac, resulting in a more sustained absorption. Subconjunctival injection is a useful form of drug delivery, particularly in serious corneal and intraocular infections.
The drug diffuses mainly through the cornea of the eye and higher intraocular concentrations may be achieved than with topical drops or ointments. The maximum volume of injected drugs usually restricted to 1 ml.
An ideal topical antibiotic should not be related to an oral drug and should be restricted to topical use only. It should have broad enough spectrum of activity to be used as a single agent.
Topical antibiotics are used to treat bacterial conjunctivitis, blepharitis and keratitis (corneal ulcers). They are also used as adjunctive treatment in cases of endophthalmitis and prophylactically to prevent infection before and after ophthalmic surgery.
Treatment is usually empirical and should have activity against the common etiological agents namely, Staphylococcus aureus, coagulase negative staphylococci, Streptococcus species, Haemophilus. Although most cases of acute bacterial conjunctivitis may resolve spontaneously, anti-infective treatment shortens the infectious process and prevents complications.
Less than 5% of medication instilled via eye drops enters the systemic circulation. Topical administration of antimicrobials has the advantage of applying the medication directly to the site of infection. The relative degree of water and lipid solubility determines the penetration of eye drops. Absorption through the corneal epithelium requires fat solubility, and water solubility is required for diffusion through the corneal stroma into the anterior chamber.
The minimum inhibitory concentration (MIC) is defined as the lowest concentration of an antimicrobial that will inhibit visible growth of an organism. The MIC for antibiotics is often expressed as the MIC90 – the concentration of antibiotic needed to inhibit 90% of a bacterial isolate.
Generally, bacteria are considered to be sensitive to an antibiotic if the achievable serum level is four times the MIC. However, bacteria reported as resistant because of lower achievable concentrations in serum may be susceptible when the medication is used topically because of the higher achievable concentration with frequent topical dosing.
Bacteria can develop resistance to antibiotics by four main methods: • They can alter the composition of their cell walls, thus creating a barrier to entrance of the medication. • The bacteria can up regulate active transport mechanisms to remove pharmacologic agents from the cell. • The bacterial target enzyme can be altered to prevent the action of the antimicrobial • The induction of or de novo development of a bacterial enzyme that can deactivate or neutralize the drug.
Aminoglycosidesare potent bactericidal agents. They have no useful activity against streptococci, anaerobes, or intracellular bacteria. They inhibit bacterial protein synthesis through interference with translation of mRNA at the ribosomal level. Clinically important aminoglycosides include gentamicin, tobramycin, neomycin, amikacin, and streptomycin. Of these, tobramycin, gentamicin and neomycin are by far the ones most commonly used in ophthalmology.
Neomycin is produced by different species of Streptomyces. Gentamicin and Amikacinaresemisyntheticaminoglycosidepreparations. Resistance to aminoglycosides occurs when the drugs fail to penetrate the cytoplasm of the organism.
Since penetration of the bacterial cytoplasmic membrane is an oxygen-dependent, active process, strictly anaerobic bacteria and facultative bacteria under anaerobic conditions are highly resistant. Bacteria can also become resistant to aminoglycosides by the production of enzymes that inactivate or destroy these agents.
Aminoglycosides are used topically for treatment of bacterial conjunctivitis, bacterial keratitis and infections of the external eye and its adnexa caused by susceptible gram-negative bacteria and pseudomonas. They have little activity against anaerobic organisms and gram-positive bacteria.
Most gram-negative organisms that possess plasmid-mediated aminoglycoside modifying enzymes will be resistant to both gentamicin and tobramycin. However, bacterial susceptibility studies demonstrate that in some cases, microorganisms resistant to gentamicin retain susceptibility to tobramycin.
Because of achemical modification, amikacin is protected from aminoglycoside inactivating enzymes and thus is the preferred drug for treatment of gram-negative infections in which resistance to both gentamicin and tobramycin occurs. In cases of bacterial conjunctivitis, commercially available gentamicin, tobramycin or amikacineyedrops may be instilled four times daily.
However, bacterial corneal ulcers require significantly higher concentrations of topical drops than are commercially available along with frequent dosing every 30 to 60 minutes. Highly concentrated, fortified preparations can be prepared, from intravenous preparations, soon before use, due to a limited shelf-life.
Neomycin, the oldest of the ocular aminoglycosides, is rarely used alone, but is widely used as prophylaxis in combination with corticosteroids following ocular surgery. Neomycin possess antiprotozoal activity and is normally used in combination with other agents in the treatment of Acanthamoeba keratitis. Topical ocular application of neomycin frequently results in sensitization to the drug, which can lead to contact dermatitis in approximately 4% of patients.
Tobramycin is marketed as a 0.3% ophthalmic solution and ointment. Like the others in this class, it has a broad spectrum. It is slightly more effective than gentamicin, especially against Pseudomonas aeruginosa. Another benefit of tobramycin is that it is less toxic than gentamicin. Though bacteria are developing increased resistance to it, tobramycin is still the drug of choice for many ocular infections.
Chloramphenicol a broad spectrum bacteriostatic antibiotic was introduced into clinical use in 1948. Originally isolated from Streptomycesvenezuelae, it is now mainly produced synthetically. It is highly active against most gramnegative and gram-positive pathogens, Rickettsia and Mycoplasma.
Enterobacteriaceae show variable resistance and Pseudomonas aeruginosa and mycobacteria are usually resistant.8 Chloramphenicol inhibits protein synthesis by reversibly binding to the 50S ribosomal subunit of bacteria, and, to a lesser degree, to mammalian cells. Chloramphenicol appears to prevent the binding of the amino acid containing tRNA to the acceptor site on the 50S ribosome
Due to the reversible binding, chloramphenicol is bacteriostatic. Chloramphenicol is an ideal drug for topical use. It penetrates well into the aqueous humor after topical application, has low ocular surface toxicity, and relatively low rates of development of resistance. It is the gold standard for the treatment of conjunctivitis against which other topical treatments are tested. Bone marrow hypoplasia including aplastic anemia and death has been reported following systemic administration, but topical chloramphenicol does not appear to present such a substantial risk.
Chloramphenicol is particularly effective against Haemophilusinfluenzae and topical preparations are used to treat infections caused by H. influenzae, S. aureus, Streptococcus species including S. pneumoniae, E. coli, Klebsiella, Enterobacter, Neisseria and Moraxella species. The usual dose of chloramphenicol solution is 1% drop to the affected eye 2 to 4 times a day or as often as advised or 1% ointment placed in the lower conjunctival sac every 3 hours or less.1
Polymixin B Sulfate Polymixin B sulfate is a polypeptide antibiotic derived from B. polymyxa. It has a bactericidal action against almost all gram-negative bacilli except the proteusgroup. All gram-positive bacteria, fungi, and gram negative cocci including N. gonorrhoae and N. meningitidis are resistant. Polymixins increase the permeability of bacterial cell membranes. Topical or subconjunctival administration of polymixin B is useful for treating acute infections caused by susceptible strains of Pseudomonas aeruginosa. he drug is contraindicated in persons with a prior history of hypersensitivity reactions to the polymixin
chlortetracycline Since the discontinuation of tetracycline eyedrops and ointment, chlortetracycline eye ointment is the only tetracycline available for topical ocular use. Derived from Streptomycesaureofaciens, chlortetracycline is a broad spectrum, bacteriostatic antibiotic effective against a wide range of bacteria. Amongst the gram-positive organisms, Streptococcus pneumoniae is susceptible to chlortetracycline.
It also inhibits coliforms, Haemophilus species, Neisseriaspecies and most other gram-negative organisms except Pseudomonas aeruginosa. Since it is actively concentrated within phagocytes, chlortetracycline is useful against intracellular pathogens such as Chlamydia and is used in the treatment of trachoma (in conjunction with oral therapy). For topical use, the ointment (1%) is applied to the affected eye every 2 hours or more frequently as indicated by the severity of infection and the degree of the response.
Fluoroquinolones In 1963, nalidixic acid was discovered during chloroquine synthesis and was noted to have antibacterial properties, but it was excreted too quickly to have any significant systemic antibacterial effects. This problem was solved in 1967,however, by fluorinating the quinolones, which gave these compounds far greater antibacterial activity, therapeutic blood levels, and low toxicity. Fluoroquinolones are bactericidal and inhibit bacterial DNA synthesis by blocking the action of two of the topoisomerase enzymes, which are present only in bacteria. Topoisomerase II, also known as DNA gyrase, allows the uncoil ingandsupercoiling of double-stranded DNA, and topoisomearse IV cleaves the doubled DNA of replicating DNA, allowing daughter cell formation. Bacteria can develop resistance to fluoroquinolones by altering their target enzymes, altering the permeability of the drug into the organism, increasing efflux pumps, and upregulating a gene conferring quinolone resistance.
Second- and Third-Generation Fluoroquinolones The second-generation fluoroquinolones include ciprofloxacin and ofloxacin, which have broad-spectrum coverage against gram-positive and gram negative bacteria. The initial ophthalmic use of the fluoroquinolones was totreat corneal and conjunctival infections; however, they have also gained wide acceptance in the prophylaxis of bacterial endophthalmitis after intraocular
Ciprofloxacin, a second-generation fluoroquinolone, was approved in 1990 and is a solution of ciprofloxacin 0.3% with 0.006% BAK as a preservative and a pH of 4.5. Ofloxacin, a second-generation fluoroquinolone, contains ofloxacin 0.3% and 0.005% BAK and has a pH of 6.4.3 Ofloxacin has a greater solubility at neutral pH than ciprofloxacin allowing it to be constituted at a more physiologic pH and permitting less drug precipitation. Because ofloxacin is more lipophilic than ciprofloxacin, it has greater penetration through the corneal epithelium. Ciprofloxacin has a lower solubility at neutral pH, which can lead to corneal precipitates.
Levofloxacin, the L-isomer of ofloxacin, is considered a third-generation fluoroquinolone. It has a higher solubility at neutral pH, allowing for a higher concentration of medication, 0.5%. It has a pH of 6.5 and is preserved with 0.005% BAK. Adverse reactions to topical second-and third-generation fluoroquinolones are mild and include discomfort, chemosis, hyperemia, eyelid edema, and punctate epithelial keratitis. Ciprofloxacin and ofloxacin are both indicated for treatment of corneal ulcers and bacterial conjunctivitis as follows
Corneal Ulcers Ciprofloxacin Two drops every 15 minutes for the first 6 hours and then two drops into the affected eye every 30 minutes for the rest of the first day. On the second day, use two drops every hour and then use 2 drops every 4 hours for the consecutive days of treatment. Ofloxacin One to two drops every 30 minutes while awake and one to two drops once during the night for 2 days. For days 3 through 7 of treatment, use drops hourly, and then four times a day for the remainder of the treatment. Bacterial Conjunctivitis Ciprofloxacin—one to two drops every 2 to 4 hours for 2 days and then every 4 hours for 5 days. Ofloxacin—one to two drops every 2 to 4 hours for 2 days and then every 4 hours for 5 days.
Different studies investigating the aqueous humor penetration of ofloxacin and ciprofloxacin in various clinical settings have shown that ofloxacin has a consistently higher penetration into the aqueous humor as compared to ciprofloxacin, although the difference was not always statistically significant. Despite the greater penetration of ofloxacin, ciprofloxacin has higher antimicrobial activity (lower MIC90) than ofloxacin for most pathogens. Ciprofloxacin has also been shown to reduce the bacterial flora on human conjunctiva severely within 15 minutes, with an antimicrobial effect lasting at least 2 hours, whereas ofloxacin did not result in a significant reduction in bacterial flora.
The recently introduced fourth-generation fluoroquinolones, gatifloxacinand moxifloxacin, have shown enhanced spectrum and potency for gram positivebacteria in addition to retaining an equal efficacy against gram-negative bacteria as the earlier fluoroquinolones.
This is because the fourth-generation fluoroquinolones bind effectively to both topoisomerases II and IV, in contrast to the older fluoroquinolones which bind more strongly to topoisomerase II, an enzyme more important for gram-negative bacteria.
Moxifloxacin and gatifloxacin penetrate well into the anterior chamber and achieve levels in excess of the MIC90 for most pathogenic organisms. For topical use, they are available as moxifloxacin 0.5% and gatifloxacin 0.3% solution. They play an important role in the treatment of bacterial conjunctivitis and keratitis and in the perioperative prophylaxis against endophthalmitis.
Like antibiotics, preservatives are divided into 2 classes: bacteriostaticandbactericidal. Though having similar classification, antibiotics are formulated to affect specific organisms, while preservatives act against all cells. In either situation, bacteriostatic substances act to inhibit the growth of the cell, while bactericidal substances inhibit cell reproduction or kill the cell outright.
Benzalkonium chloride remains one of the most popular bacteriocidal preservatives. Although it can be rather toxic, this serves to enhance drug penetration.
In the field of artificial tears, there has been a focus on the development of less irritating preservatives. For instance, sodium perborate is used in Genteal. This agent is unique in that contact with the eye changes it into oxygen and water, producing minimally-lasting negative effects.
Purite (in Refresh) and Polyquaternium-1 (in Systane) are other new additions to the line of artificial tears preservatives.
Vehicles are inert (nonactive) agents that either provide support for or are used to dissolve the active drug. Though they may be used as a buffer, their major function is to control viscosity (thickness) of the solution. Increasing the viscosity increases the contact time of the active drug. Some commonly used vehicles in ophthalmic solutions are povidone (PVP), polyvinyl alcohol, and carboxymethylcellulose.