Download
1 / 16
240 likes | 848 Views
1. A 2-cm gastric ulcer in the antrum of the stomach is associated with all of the following EXCEPT H. pylori infection Increased acid secretion Malignancy NSAIDs Atrophic gastritis. 1. Answer B Gastric ulcer classification I (50%): body/antrum of stomach, along lesser curvature

E N D
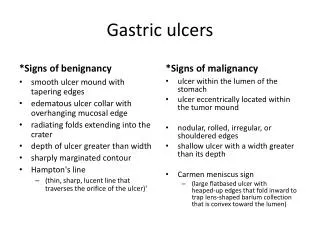
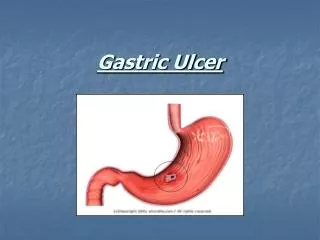
1. A 2-cm gastric ulcer in the antrum of the stomach is associated with all of the following EXCEPT • H. pylori infection • Increased acid secretion • Malignancy • NSAIDs • Atrophic gastritis
1. Answer B • Gastric ulcer classification • I (50%): body/antrum of stomach, along lesser • curvature • Low to normal acid levels • Tx with antrectomy • II (25%): type I + duodenal ulcer • High acid levels • Tx with vagotomy, antrectomy • III (15%): prepyloric • High acid levels • Tx with vagotomy, antrectomy • IV: close to GE jxn • Low to normal acid levels • V: anywhere in stomach, drug-associated
2. A generally healthy 35-year-old man has a 6-hour history of abdominal pain and nausea. He passes a stool containing mucous and blood. A CT scan is obtained and shown below. • The best therapeutic intervention would be • a. colonoscopy • b. IV neostigmine • c. Barium enema • d. Bowel resection and anastamosis • e. Nasogastric suction and antibiotics
3. The most common cause of this condition in adults is a. Meckel’s diverticulum b. Gallstones c. Ischemic bowel disease d. Crohn’s disease e. Gastrointestinal tumor
2. Answer D 3. Answer E Intussusceptum: proximal portion that invaginates into distal bowel Intussuscipiens: recipient, distal bowel into which proximal bowel invaginates into Children: under 3 years old, preceded by nonspecific febrile illness (viral), hypertrophy of Peyer’s patches Adults: malignancy (lymphoma) Dx: CT scan Tx: resection
4. A 58-year-old woman has had no flatus or bowel movement for 2 days, and intermittent vomiting for the past 24 hours. She has had mid-epigastric pain for the past 3 years, but has never sought treatment. Diet modification helped decrease the frequency and severity of pain. She has never had a previous abdominal operation. Exam demonstrates a distended abdomen with moderate tenderness to deep palpation but no rebound. No stool or masses are noted on rectal exam. An abdominal x-ray is shown. The most likely etiology is a. tuberculosis b. fungal c. inflammatory d. neoplastic e. bacterial
5. The patient is taken to the OR and exploration reveals the finding shown. The management of choice is a. enterotomy b. adhesiolysis c. segmental resection d. peritoneal washings e. intestinal bypass
4. Answer C 5. Answer A Rigler’s triad: abd xray -- SBO, pneumobilia, radioopaque stone Xray often non-diagnostic • Etiology: recurrent cholecystitis with inflammtion and adhesion formation, stone erodes through gallbladder into adjacent viscus, usually duodenum • Distal ileum common site of obstruction • Tx: resuscitation, OR enterotomy proximal to stone • Not necessary to deal with cholecystoenteric fistula at initial operation, spontaneously close in many • Elective cholecystectomy • Recurrence rate 5%
6. A previously healthy 25-year-old woman has right lower quadrant pain and fever. CT confirms appendicitis. After an uneventful appendectomy, the patient is discharged. The final report on CT describes a 2.0 cm left adrenal mass.The patient is asymptomatic. Which of the following is NOT appropriate?a. dexamethasone suppression testb. measurement of serum potassium and plasma aldosterone concentration/plasma renin activity ratioc. fine-needle aspiration biopsyd. adrenalectomy if the tumor is functionalfollow-up CT in 6 to 12 months
6. Answer C Adrenalectomy for lesions > 6 cm Nonfunctioning lesions < 4 cm interval CT or MRI at 6 months and 1 year 4-6 cm adrenalectomy or close observation 90% benign · r/o subclinical hypercortisolism · 1-mg dexamethasone suppression test overnight · 8 AM plasma cortisol > 3 mg/dL (failure to suppress) · chk 24-hour urinary free cortisol and plasma ACTH ·Aldosteronoma least common · screened for only in patients with HTN or hypokalemia · serum potassium, plasma aldosterone/plasma renin (>20) · confirm with 24-hour urinary aldosterone levels
· Pheochromocytoma · fractionated urinary and/or plasma catecholamines, metanephrines, and urinary vanillylmandelic acid (VMA) · Preoperative α-adrenergic blockade with phenoxybenzamine - administered for at least 1 week before operation - Side effects: reflex tachycardia, nasal congestion · intravenous fluids · β-Adrenergic blockade for reflex tachycardia - do not give until adequate α-blockade established
7. A 43-year-old man with alcoholic cirrhosis has had two episodes of variceal hemorrhage treated acutely with sclerotherapy. Lab values are as follows: albumin 3.3 g/dL; total bilirubin 1.2 mg/dL, alkaline phosphatase 120units/mL, PT 12 sec (control 11.5 sec), PTT 36 sec, aspartate amino transferase 30 units/L, and alanine amino transferase 25 units/L. He has no ascites and has never been encephalopathic. Appropriate management at this time might include each of the following EXCEPT a. distal spleno-renal shunt b. endoscopic rubber band ligation c. transjugular intrahepatic portosystemic shunt d. orthotopic liver transplantation e. small diameter H portocaval shunt
Score Ascites (grade) Bilirubin (mg/dl) Albumin (gm/dl) PT (sec prolonged) Hepaticencephalopathy 1 None < 2 > 3.5 < 4 None 2 Mild 2 - 3 2.8 - 3.5 4 - 6 1 - 2 3 Severe > 3 < 2.8 > 6 3 - 4 7. Answer D Pt is Child’s class A Child’s-Pugh Classification (A BATH) A 5 – 6 Life expectancy: 15 to 20 years, abdominal surgery peri-operative mortality: 10% B 7 – 9 Indicated for liver transplantation evaluation, abdominal surgery peri-operative mortality: 30% C > 9 Life expectancy: 1 to 3 years, abdominal surgery peri-operative mortality: 82%
Management of variceal bleedings Acute: Octreotide, endoscopic ligation, sclerotherapy, balloon tamponade, TIPS
Portosystemic shunts • Nonselective shunts: more encephalopathy • End-to-side portacaval: all portal flow diverted intosystemic circulation, ascites persists • Side-to-side portacaval, interposition (16 mm), splenorenal: better at controlling ascites b/c splanchnic venous and intrahepatic sinusoidal drainage still open • Selective • Distal splenorenal shunt: Distal splenic vein to left renal vein, ligate collateral veins, can worsen ascites • Partial shunts • Meso/Portacaval interposition with small-diameter (8 mm) graft, maintains hepatic portal perfusion