Download
1 / 48
480 likes | 658 Views
Philippe G Jorens Department of Critical Care Medicine University of Antwerp, Antwerp University Hospital , Belgium. Answering the call of nature Fluid strategy in traumatic brain injury . 2012. 1. Physio pathogenesis of TBI . Primary injury

E N D
Philippe G JorensDepartment of Critical Care MedicineUniversity of Antwerp, Antwerp University Hospital , Belgium Answering the call of nature Fluid strategy in traumatic brain injury 2012
1. Physio pathogenesis of TBI • Primary injury • physical damage to the parenchyma during the insult • shearing and compression • Secondary injury • complex process • edema • (Webster’s dictionary) • an abnormal collection of watery fluid in a bodily tissue or cavity
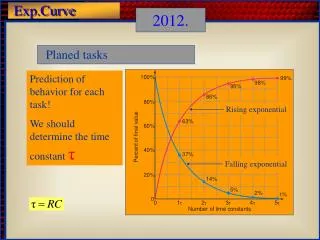
Ropper 2012 ICP and edema determine outcome The cranium is a fixed vault … Brain parenchyma = 80 % water: brain volume is responsive to changes in water content CPP = MAP – ICP
Your brain is precious • Keep it dry …
Blood-brain barrier • Lund concept • Heterogeneous disruption of the protective blood-brain barrier • Starling equation is used • Reduction of arterial and venous intravascular pressure • Supplementing oncotic pressure with albumin
What happens in our patients with TBI ? • Hypotension (defined as SBP < 90 mm hg) • MAP < 65 mm Hg • Occurs 73 % during ICU stay (Chesnut et al. 1993) • Independent predictor of severe outcome ( Chesnut et al, 1993b): doubling mortality • Most amenable to prevention • Intravascular volume depletion usually due to • Associated hemorrhage • Drugs we use (etomidate) • Myocardial contusion • Hypovolemia and hypoosmolarity worsen brain edema
Answer the call of nature • Webster’s dictionary • (= pass liquid from the body)
What should we do ? • Aggressive fluid administration • CVP 8 – 10 mm Hg • Monitor (PCWP 12 -15 mm Hg) • Excessive and inappropiate • Fluid overload and ARDS • Large amounts of fluids can be administered in most TBI patients
Which fluids should we use ? • Crystalloid-based fluid strategies are favored • But evidence in brain injury is limited • Pragmatic approach to resuscitation …
A Comparison of Albumin and Saline for Fluid Resuscitation in the Intensive Care Unit The SAFE Study Investigators N Engl J Med Volume 350;22:2247-2256 May 27, 2004
Study Overview • In critically ill patients, both albumin and saline are commonly used for fluid resuscitation, but it is unknown whether one intravenous fluid is superior to the other • In this clinical trial in critically ill patients in the intensive care unit, the use of albumin and saline resulted in similar outcomes at 28 days • Because the two treatments are equivalent with respect to clinical outcomes, the decision about which fluid to use should be determined by physician preference, safety, and cost
Kaplan-Meier Estimates of the Probability of Survival The SAFE Study Investigators, . N Engl J Med 2004;350:2247-2256
Relative Risk of Death from Any Cause among All the Patients and among the Patients in the Six Predefined Subgroups The SAFE Study Investigators, . N Engl J Med 2004;350:2247-2256
Conclusions • In patients in the ICU, use of either 4 percent albumin or normal saline for fluid resuscitation results in similar outcomes at 28 days
Original ArticleSaline or Albumin for Fluid Resuscitation in Patients with Traumatic Brain Injury The SAFE Study Investigators N Engl J Med Volume 357(9):874-884 August 30, 2007
Study Overview • In this study of 460 patients with traumatic brain injury, a post hoc analysis of a larger randomized trial comparing saline and albumin for fluid resuscitation in patients requiring intensive care, the mortality rate was significantly higher in the albumin group • These findings suggest that albumin should not be used for fluid resuscitation in patients with severe traumatic brain injury
Enrollment of Patients and Assessment of Primary Outcomes The SAFE Study Investigators. N Engl J Med 2007;357:874-884
Baseline Characteristics of the Patients The SAFE Study Investigators. N Engl J Med 2007;357:874-884
Fluids Administered and Physiological Effects of Treatment The SAFE Study Investigators. N Engl J Med 2007;357:874-884
Primary and Secondary Outcomes The SAFE Study Investigators. N Engl J Med 2007;357:874-884
Kaplan-Meier Estimates of the Probability of Survival The SAFE Study Investigators. N Engl J Med 2007;357:874-884
Conclusion • In this post hoc study of critically ill patients with traumatic brain injury, fluid resuscitation with albumin was associated with higher mortality rates than was resuscitation with saline
Guidelines …. • Reinhart et al. Intensive Care Med 2012 • Consensus statement on colloid volume therapy as interpreted by the respective ESICM task force. • No colloids should be used in patients with head injury …
Houston, we have a problem … Albumin 4 %
Rohling-Waldstrom et al. 2009Albumin 4 and 20 % Albumin 4 and 20 %
Hypertonic or hyperosmolar solutions ? • Mannitol • causes ICP decrease by the elimination of water • Osm 310-320 mosm/kg • Compensated by adequate fluid replacement … • Problem list: cause a reverse osmotic shift, raising brain osmolarity (Wise et al. 1964) • HSS • increasing salt • expands intravascular volume (Para et al. 2010) • Improves rheology
Hays et al. 2011 The lack of scientific evidence leads to heterongeneous practice patterns . Hays et al. 2011
We have not listened to the call of nature … • Albumin BB
We have used the wrong endpoints .. • SAFE: • evaluation albumin directed to hemodynamic/resuscitation endpoints , not the posssible benefits of maintaining serum albumin during ongoing care • Hyperosmolar agents remove fluid from the remaining normal brain tissue : little effect on the damaged brain • Once hyperosmolarity has been attained, it must be sustained • Albumin in stroke (ALIAS)
We have forgotten how to calculate … • Normal plasma osmolality • normal plasma osmolality = 285 mosm/kg. • Plasma proteins account only for 1 mOsm/kg • A reduction in COP has little effect on total osmolality • But a reduction of 5 mOsm/kg has an enormous effect on water movements • Osmolarity= sum (in-vitro) of all particles with potential osmotic acitivity
Van Aken et al. 2012 This means: human albumin 4% , gelatine and Hartmann’s solution: low measured in-vitro osmolality That no colloids should be used in patients with TBI is not supported by physiological principlis: rather … hypo-osmolar/hypotonic solutions should be avoided …
Two forms of edema … • Vasogenic edema • Breakdown BBB • Along white-matter tracts : spares cortical gray matter • Contusion, inflammation, subacute phase of cerebral infarction • Cytotoxic edema: • Ischemia: reduction of ATP production • Cellular swelling • Hyperacute ischemic infarction • Gray and white matter
Confused … • We want to keep the brain dry
Confused … • We want to perfuse the brain
Conclusion • Large amounts of fluids can be used in TBI • Colloids should be used with caution • Avoid hypotonic solutions • Albumin ? • Hypertonic solutions can be used