Download
1 / 1
10 likes | 106 Views
Case of the week 08-02: apical HCM, fibrosis and sustained VT. History: An 82 yr ♂ admitted with palpitations, presyncope and sustained monomorphic VT. Family history, his brother died age 6 of unknown cause. Echo: LVH. Referred for CMR for further clarification.

E N D
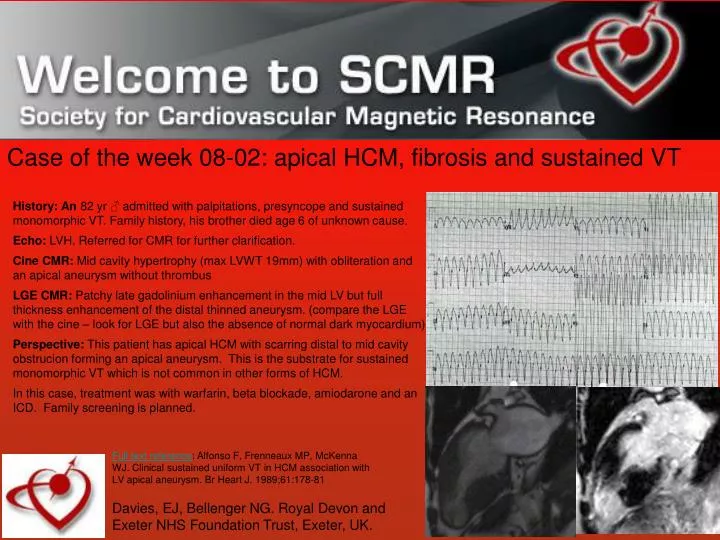
Case of the week 08-02: apical HCM, fibrosis and sustained VT History: An 82 yr ♂ admitted with palpitations, presyncope and sustained monomorphic VT. Family history, his brother died age 6 of unknown cause. Echo: LVH. Referred for CMR for further clarification. Cine CMR: Mid cavity hypertrophy (max LVWT 19mm) with obliteration and an apical aneurysm without thrombus LGE CMR: Patchy late gadolinium enhancement in the mid LV but full thickness enhancement of the distal thinned aneurysm. (compare the LGE with the cine – look for LGE but also the absence of normal dark myocardium) Perspective: This patient has apical HCM with scarring distal to mid cavity obstrucion forming an apical aneurysm. This is the substrate for sustained monomorphic VT which is not common in other forms of HCM. In this case, treatment was with warfarin, beta blockade, amiodarone and an ICD. Family screening is planned. Full text reference: Alfonso F, Frenneaux MP, McKenna WJ. Clinical sustained uniform VT in HCM association with LV apical aneurysm. Br Heart J. 1989;61:178-81 Davies, EJ, Bellenger NG. Royal Devon and Exeter NHS Foundation Trust, Exeter, UK.