Download
1 / 50
570 likes | 794 Views
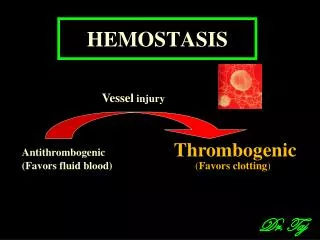
HEMOSTASIS. Spontaneous arrest of bleeding by physiological process in an injured blood vessel. Prevents the blood loss, maintains the blood in fluid state. More effective in small vessel. Mechanism : Vascular spasm / blood vessel constriction .

E N D
Spontaneous arrest of bleeding by physiological process in an injured blood vessel. Prevents the blood loss, maintains the blood in fluid state. More effective in small vessel
Mechanism : • Vascular spasm / blood vessel constriction . • Formation of platelet plug. • Formation of a blood clot. • Eventual growth of fibrous tissue in to the clot.
BV Injury Contact/ Tissue Factor Neural Platelet adhesion, activation and release, Aggregation Coagulation Cascade BloodVessel Constriction Primaryhemostatic plug Reduced Blood flow Platelet Activation Fibrin formation Stable Hemostatic Plug
VASCULAR SPASM / CONSTRICTION : -Trauma to the blood vessel. Reduce the blood loss , platelets remains longer at the site of injury Results from: Nervous reflexes Local myogenic spasm Local humoral factors Eg: 5-HT, Thromboxane A2
platelet: Plasmamembrane: specific receptors –repels normal endothelium. Contractile proteins: Actin ,Myosin, Thrombosthenin. Mitochondria : ATP & ADP. Lipids: Prostaglandins, Tromboxane. Endoplasmic reticulum & Golgi Apparatus : Enzyme synthesis. Protein : fibrin stabilizing protein. Granules • Alpha : Fibrinogen, Von -Willebrand Factor(VWF), factors v, Factors vii. • Dense: ADP,ATP,5-HT, Ca 2+.
2. MECHANISM OF PLATELET PLUG FORMATION: a. Platelet adhesion: exposed collagen Von -Willebrand Factor - Released from Endothelial cells and platelets .
b. Platelet activation and release: PAF • Platelets activated by adhesion. • Swells, numerous pseudopod like projections from the surface. • Extend projections to make contact with each other. • Contractile proteins thrombospondin and thrombonectincontracts forcefully. • Serotonin
Increase ADP, Thromboxane A2 release- activate other platelets. • Membrane phospholipids rearrange. • Ca 2+ release. • Serotonin/ 5-HT & Thromboxane A2 are vasoconstrictorsdecreasing blood flow through the injured vessel. ADP causes stickiness.
c.Platelet Aggregation:PAF ADP + Thromboxane A2 Activate, Increase the stickiness of additional platelets loose platelet plug
3.Formation of blood clot. Procoagulants . Anticoagulants. Balance b/w Procoagulants and anticoagulants keep the blood in fluid state .
Mechanism of clotting: Cascade of reaction In which inactive clotting factors are activated and this in turn activate other inactive clotting factors = Water Fall Hypothesis blood is transformed from a liquid to a gel state.
Clotting factors Factor 1 – Fibrinogen. Factor 2 – Prothrombin. Factor 3 –Tissue Thromboplastin. Factor 4 – Calcium Ion. Factor 5 -- proaccelarin. Factor 6 - Absent . Factor 7 – proconvertin. Factor 8- Anti Hemophilic factor. Factor 9- Christmas Factor. Factor 10 – Stuart Prower factor. Factor 11-plasma thromboplastin antecedent Factor 12- Hageman Factor. Factor 13- Fibrin Stabilizing Factor.
Other factors : Heavy molecular weight Kininogens. Kallikreins. Pre Kallikreins. Platelet Phospholipids.
The final three steps of this series of reactions are: • Prothrombin activatoris formed. • Prothrombin is converted into thrombin. • Thrombin catalyzes the conversion of fibrinogen into a fibrin mesh.
Prothrombin Activator 2 Pathways : Intrinsic Pathway Extrinsic Pathway
Intrinsic pathway Invivo : Inactive clotting factor XII is activated by surface contact with collagen. Change in blood constituents. Invitro: Blood exposed to glass materials
Extrinsic pathway– Activated by tissue factor/tissue thromboplastin. Injury to vessel wall. Injury to body tissue. Tissue thromboplastin is not a plasma protein – released from outside the endothelium ( Damaged tissue )
Intrinsic system Extrinsic system HMWK,KK XII XIIa Tissue thromboplastin HMWK XI XIa VII VIIa Ca2+ IX IXa VIII VIIIa PL, ca2+, Ca2+,Factor III,PL X Xa X Ca2+ PL V Va Prothrombin Thrombin Fibrinogen Fibrin Ca2+,PL XIIIa XIII
Conversion of Prothrombin to Thrombin Prothrombin Thrombin Formation of Fibrin *Prothrombin activator polymerization Fibrinogen(soluble) Fibrin( Monomer) Proteolysis Stabilization Stabilized Fibrin(Polymer) Insoluble Fibrin (Polymer) Ca2+ XIII XIII (a)
4. CLOT RETRACTION: 1 hour50% of the clot retracts. Impaired if platelets are decreased or absent. Clot retracts – pulls the broken vessels together, facilitates wound healing and prevents thrombolysis
Injury to the vessel wall Release of factor III Endothelium disrupted –collagen exposed Release of 5-HT & other vasoconstrictors Via extrinsic system Via intrinsic system Platelet adhesion Constriction of injured blood vessel Activation of coagulation Platelet activation Formation of fibrin Platelet aggregation Formation of temporary platelet plug Formation of a definitive hemostatic plug
FIBRINOLYSIS : • Vascular endothelium release of thrombomudulin Thrombomodulin + Thrombin Protein C activated Protein C with protein S activation of Inactivates Va and VIII a plasminogen activator
Fibrin/ Fibrinogen Tissue plasminogen activator plasmin plasminogen Fibrin degradation products
Why blood does not clot in the blood vessels???? • Endothelial factors: Smoothness of the endothelium. Negatively charged particles on the endothelium. Thrombomodulin. 2. Velocity of blood circulation. 3. Presence of natural anticoagulants. Eg: Heparin , Protein C, Protein S 4. Negative feed back by thrombin
ADP + Thromboxane A2 Prostacyclin &NO Prostacyclin & NO Vessel injury
Applied Aspects : • Vit K deficiency Factor II ,Factor VII ,Factor IX ,Factor X , protein C. • Diseases of Liver • Gastro intestinal disease • Decrease in dietary Vit K. Treatment: Injecting Vit K
2. Hemophilia : It’s a clotting disorder caused due to the deficiency of the clotting factors Hemophilia A – deficiency of Factor VIII (85%) Hemophilia B – deficiency of Factor IX (15%) Hemophilia C – deficiency of Factor XI (Rare)
First detected among the British royal family members- Royal disease. Sex linked disorder –abnormal gene on the X-chromosome. Females are the carriers( No symptoms) and males the sufferers /manifest signs of the disease. Presence of another normal X chromosome ,the gene acts as a recessive gene.(no signs of disease but can transmit the disease)
Bleeding time : Time from the onset of bleeding to the formation of the temporary platelet plug . Normal value: 2-5 min. Clotting time: Time from the onset of bleeding to the formation of the first Fibrin thread. Normal value: 3 -8 min Diagnosis: • Increase in clotting time . • Bleeding time is normal
Carrier Female Normal Male Y X X X X X Y X X X X Y Normal Female Carrier female Hemophilic male Normal male
Treatment: • Fresh blood transfusion Factor VIII is lost rapidly on storage. • Injecting factor VIII,IX prepared from fresh frozen plasma.
3. Platelet disorder: A. Thrombocytopenia: Reduction in the platelet count secondary to some other cause. B . Idiopathic thrombocytopenia: Reduction in the number of platelets due to unknown cause. C. Thromboasthenia : Defective platelet function.
Hyper coagulable disorder: Clot appear spontaneously in the vessels and heart-:Thrombosis Thromboembolism: clot blocks the smaller vessels. Causes: Antithrombin III deficiency , protein C deficiency, plasminogen abnormalities etc Risk factors : Atherosclerosis, hyperlipidaemia , slow blood flow, smoking etc
4.Defective capillary contractility: The clinical condition in Which the capillary abnormality results in bleeding is called PURPURA. Characterized by spontaneous haemorrhages beneath the skin, mucous membrane and internal organs.
Types: Primary (idiopathic) - congenital or hereditary and usually occurs in children. Secondary (symptomatic) - due to allergies, infection.
Thrombocytopenic Purpura: low platelet count. • Mild: less than 50,000 cells/cumm of blood. • Moderate: less than 10,000 cells /cumm of blood. • Fulminating : less than 1000 cells/cumm of blood
Purpura develops in following condition: • Increase capillary fragility • Thrombocytopenia • Idiopathic thrombocytopenia • Thromboasthenia • Allergy, drug toxicity
ANTICOAGULANTS Natural anticoagulants Heparin Protein-C, Protein S Synthetic anticoagulants: Heparin Vit K antagonists EDTA, Sodium citrate Oxalates Aspirin
Synthetic Anticoagulants: 1.Heparin: ( In Vivo & In Vitro ) Administered after surgery to avoid thrombosis 2.Aspirin: Inhibit platelet aggregation 3.Vitamin K Antagonists: Dicoumarol, Warfarin
Synthetic Anticoagulants( In Vitro) • Heparin • Oxalates & Citrates & EDTA Decreases the conc. of Ca ions in the blood
Prostacyclin & NO Prostacyclin & NO ADP Thromboxane A2 Vessel injury