Download
1 / 34
390 likes | 975 Views
Modes of Mechanical Ventilation. Mohamad S Ahmad, M.D. Lecturer of Anaesthesia and Intensive CareAin Shams University Cairo, Egypt 2008. Introduction. Ventilation The goal of ventilation is to facilitate CO2 release and maintain normal PaCO2 Minute ventilation (VE)

E N D
Modes of Mechanical Ventilation Mohamad S Ahmad, M.D. Lecturer of Anaesthesia and Intensive CareAin Shams University Cairo, Egypt 2008
Introduction Ventilation • The goal of ventilation is to facilitate CO2 release and maintain normal PaCO2 • Minute ventilation (VE) • Total amount of gas exhaled/min. • VE = (RR) x (TV) • VE comprised of 2 factors • VA = alveolar ventilation • VD = dead space ventilation • VD/VT = 0.33 • VE regulated by brain stem, responding to pH and PaCO2
Oxygenation • The primary goal of oxygenation is to maximize O2 delivery to blood (PaO2) • Alveolar-arterial O2 gradient (PAO2 – PaO2) • A-a gradient measures efficiency of oxygenation • PaO2 partially depends on ventilation but more on V/Q matching
To affect oxygenation, adjust: FiO2 PEEP I time PIP To affect ventilation, adjust: Respiratory Rate Tidal Volume Adjustments VE MAP
COMPLIANCE = Volume / Pressure If volume is set, pressure varies…..if pressure is set, volume varies
Goals of MechanicalVentilation • Achieve and maintain adequate pulmonary gas exchange • Minimize the risk of lung injury • Reduce patient work of breathing • Optimize patient comfort
Ideal Mode of Ventilation • Synchronizes with the patient’s spontaneous respiratory effort • Maintains adequate and consistent tidal volume and minute ventilation at low airway pressures • Responds to rapid changes in pulmonary mechanics or patient demand • Provides the lowest possible WOB
Ideal Ventilator Design • Achieves all the important goals of mechanical ventilation • Provides a variety of modes that can ventilate even the most challenging pulmonary diseases • Has monitoring capabilities to adequately assess ventilator and patient performance • Has safety features and alarms that offer lung protective strategies
MODES • Ventilator mode can be defined as a set of operating characteristics that control how the ventilator functions • Operating mode can be described by (1)the way a ventilator is triggered into inspir. and cycled into expir., (2)what variables are limited during inspiration, (3)and whether or not the mode allows mand., spont. breaths or both. • spontaneous, PEEP, CPAP, BiPAP, CMV, AC, IMV, SIMV, MMV, PSV, PCV, APRV, IRV
SPONTANEOUS • Not an actual mode since rate and tidal volume during spont. breathing are determined by patient • Role of ventilator during spont. vent. is to provide the (1) flow to the pt. in a timely manner, (2) flow adequate to fulfill a patient’s insp. demand, and (3) provide adjunctive modes such as PEEP to complement the spont. effort • Apnea ventilation is a safety feature used for spontaneous mode
PEEP • PEEP increases the end-expiratory or baseline airway press. to a value greater than atmos. and is often used to improve the pt.’s O2 status, esp. if refractory • PEEP is not a stand-alone mode, but is used in conjunction with other modes • Two major indication for PEEP are: - Intrapulmonary shunt - Decreased FRC and lung compliance • Complications assoc. with PEEP include - Decrease venous return and C. O. - Barotrauma - Incr. ICP - Alterations of renal, hepatic blood flow
CPAP • Is PEEP applied to a spont. breathing pt. • Indications are same as PEEP but in addition pt. must have adequate lung function to sustain eucapnic ventilation • Can use in with ET tube or facemask
BiPAP • Allows one to apply IPAP and EPAP • IPAP provides positive pressure breaths and it improves hypoxemia and/or hypercapnia • EPAP (essentially PEEP) improves oxygenation by increasing the FRC and enhancing alveolar recruitment
Indications for BiPAP: - preventing intubation of end-stage COPD patient - supporting patients with chronic ventilatory failure - patient’s with restrictive chest wall disease - neuromuscular disease - nocturnal hypoventilation
CMV • Ventilator delivers the preset tidal volume at a set time interval • should only be used when the pt. is properly medicated with a combination of sedatives, respiratory depressants and neuromuscular blockers • Indicated if pt. “fights” the vent., seizure, complete rest for pt. for 24 hr., chest injury
Assist Control (A/C) • Pt. always receives a mechanical breath, either timed or assisted
Indicated when full ventilatory support is needed, used when pt. has a stable respiratory drive (10-12 spont. rate) • Advantages include a very small WOB when sens. and flow are set properly, and this mode allows the pt. to control the RR • Disadvantage include alveolar hypervent.
IMV • Pt. breaths spont. at any tidal volume between the mechanical breaths • Primary disadvantage is chance for breath stacking, therefore care should be taken to set high press. limit properly to reduce risk of barotrauma
SIMV • A mode in which the vent. delivers mandatory breaths to the pt. at or near the beginning of a spont. breath, mandatory breaths are synchronized with the pt.’s spont. efforts to avoid breath stacking
“synchronized window” refers to the time just prior to time triggering in which the vent. is responsive to the pt.’s effort (0.5 sec is typical) • Advantages include maintaining resp. muscle strength, reduces V/Q mismatch, decreases mean airway press., helps wean pt
PSV • Used to lower the WOB and augment a patient’s spont. tidal volume • When PSV is used with SIMV, it lowers the O2 consumption because of the decr. WOB • Typically used in the SIMV mode to help weaning by (1) increasing spont. tidal volume (2) decreasing spont. RR (3)decreasing WOB
PCV • The pressure controlled breaths are time triggered by a preset resp. rate • Once inspir. begins, a pressure plateau is created and maintained for a preset inspir. time • Typically used in ARDS where it takes excessive press. in volume cycled modes to ventilate a pt., leading to barotrauma
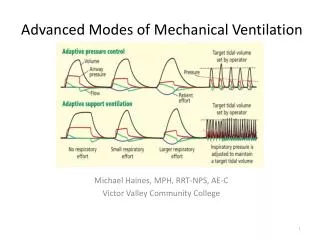
ALTERNATIVE MODES OF MECHANICAL VENTILATION • Dual-control ventilation modes were designed to combine the advantages of volume-control ventilation with pressure-control ventilation • These dual-control modes attempt to increase the safety and comfort of mechanical ventilation
pressure-regulated volume-control (PRVC) • a desired tidal volume is preset and the ventilator delivers a pressure-limited (controlled) breath until that preset tidal volume is achieved • ↑ Vt ↓ PIP & ↓ Vt ↑ PIP • provides the opportunity to deliver minimum minute ventilation at the lowest peak airway pressures possible
volume support ventilation (VSV) • The patient triggers every breath, controlling his own respiratory frequency and inspiratory time but the machine can guarantee minute ventilation • The pressure support is automatically adjusted up or down according to patient's lung compliance and/or resistance to deliver a preset tidal volume • This mode cannot be used in a patient who lacks spontaneous breathing effort • This mode is considered as a self-weaning mode
Automode PRVC VSV • designed for automatic weaning from pressure control to pressure support depending on the patient's effort
Volume-assured pressure support ventilation (VAPSV) PSV VCV • Advantages include a reduction in the work of breathing, lowered airway resistance, and lowered intrinsic PEEP
Automatic tube compensation(ATC) Designed to overcome the resistance of the endotracheal tube by means of continuous calculations
Proportional assist ventilation(PAV) • This mode adjusts airway pressure in proportion to the patient's effort • If patient's effort and/or demand are increased, the ventilator support is increased, and vice versa, to always give a set proportion of the breath
High-frequency ventilation (HFV) • HFV is time-cycled positive pressure ventilation that delivers a high frequency (60–120 breathes per min) of small tidal volumes (1.5 mL/kg) that are usually less than the anatomic dead space • 3 different modes: high-frequency positive-pressure ventilation (HFPPV), high-frequency jet ventilation (HFJV), and high-frequency oscillatory ventilation (HFOV)
APRV (airway pressure release ventilation) • Is similar to CPAP in that the pt. is allowed to breathe spont. without restriction
Combines two separate levels of CPAP and the pt. may breathe spont. from both levels • Periodically, pressure is dropped to the lower level, reducing mean airway press. • During spont. expir. the CPAP is dropped (released) to a lower level which simulates an effective expiration
Thank You