Download
1 / 8
100 likes | 511 Views
Pyogenic Spinal Infections. Pyogenic Spondylitis: Body involvement , starting in the endplates. Septic intervertebral discitis Spinal Epidural abscess. Presentation. Acute Sub-acute - common. Chronic - common Average delay in diagnosis : 8 weeks to 3 months. Presentation.

E N D
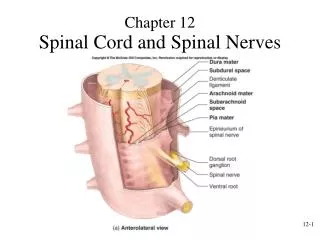
Pyogenic Spinal Infections • Pyogenic Spondylitis: Body involvement , starting in the endplates. • Septic intervertebral discitis • Spinal Epidural abscess
Presentation • Acute • Sub-acute - common. • Chronic - common • Average delay in diagnosis : 8 weeks to 3 months.
Presentation • Usually have underlying infection source. • C/o Back Pain - similar to mechanical LBP. • Fever: Only 33% >100F( Garcia, JBJS 1960) • Local tenderness may or may not be present. • Muscle spasm +/- , Psoas Abscess • Neurology in late cases. • Symptoms much more than examination findings may suggest
Diagnosis • Need a high index of suspicion. • ESR/CRP - usually high - but non-specific. • Bone scan - May be false negative( disc avascular). Or may show ‘degenerative change’ only. • MRI - Best. High signal on T2 image . • WBC count - unhelpful • Blood cultures - during fever spike. +/-.
Diagnostic pitfalls • No fever, no local tenderness. • ESR high due to other causes. • Bone scan negative. • Referred pain - abdomen,’hip’, chest. • May present with worsening of long standing mechanical low back pain. • First pass investigations may be negative in early disease.
Predisposing factors • Diabetes • Rheumatoid Arthritis • Other infections - urinary, chest, septicemia. • I/V drug abuser • Anti-cancer treatment • Long term steroid use.
Mangement • Confirm diagnosis • WBC, ESR, Blood Culture. • Percutaneous washout and biopsy in selected cases. • Antibiotics for 3 months usually
Organisms • Commonest is Staph. Aureus. • Pseudomonas in immuno-compromised hosts. • Could be Candida or TB.