Download
1 / 51
570 likes | 920 Views
SPINAL CORD, DISEASES AND DIFFERENTIAL DIAGNOSIS. Prof.Dr.Ayse ALTINTAS I.U.CERRAHPASA MEDICAL SCHOOL, NEUROLOGY DEPT. 3RD GRADE, 2011 OCTOBER. MEDULLA SPINALIS. The spinal cord, the grayish-white oblong cylindrical continuation of the medulla oblongata of the brain,

E N D
SPINAL CORD, DISEASES AND DIFFERENTIAL DIAGNOSIS Prof.Dr.Ayse ALTINTAS I.U.CERRAHPASA MEDICAL SCHOOL, NEUROLOGY DEPT. 3RD GRADE, 2011 OCTOBER
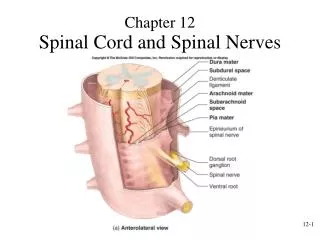
MEDULLA SPINALIS • The spinal cord, the grayish-white oblong cylindrical continuationof the medulla oblongata of the brain, • ***begins atthe foramen magnum of the skull and • ***extends within thevertebral canal to terminate as the cone-shaped conus medullaris
MEDULLA SPINALIS • In the adult the caudal tip of the conus medullaris is located between vertebral levels L1 and L2. • Thus, the adult spinal cord is approximately 45 cm in lengthwith an average diameter of 1–1.5 cm
MEDULLA SPINALIS • The spinal cord is a two-way conduit to and from the brain. • It functions as a “central relay station”, receiving incoming information fromthe body and the brain, • and as a “central processing station”, conveying outgoing information to the body and the brain.
Each spinal nerve leaves the vertebral column via its intervertebralforamen and is named accordingly. • The first eightspinal nerves, C1–C8, exit the vertebral canal above the correspondinglynumbered cervical vertebrae, whereas all subsequentspinal nerves (T1–T12, L1–L5, S1–S5, and Co1) exitbelow the correspondingly named vertebrae • Hencethere are 31 pairs of spinal nerves emerging from the spinalcord. • The region of the spinal cord associated with a particular • pair of spinal nerves is called a spinal segment.
VASCULAR SUPPLY OF THE SPINAL CORD ***Theanteriorspinalarteries,direct branches of the vertebralarteries, joinwitheachother to form a singlemedianvessel, theanteriorspinalartery, whichprovidessmallbranchesthat penetrate and supply the white and gray matter of thespinalcord.
VASCULAR SUPPLY OF THE SPINAL CORD ***The posterior spinal arteries also arise from the vertebralarteries directly or frequently indirectly by way of the inferiorcerebellar branch of the vertebral artery. **penetrate and serve the white and gray matter of thespinalcord.
SPINAL CORD • Acute spinal cord dysfunction • Can develop over seconds to week • a common reason for neurology referral
SPINAL CORD-STRUCTURE • Theneurologist’s tasks are to determine • the etiology, • institute treatment to reverse the acute deficit, • subsequentlydetermine whether there is a risk of recurrence (especially for inflammatory demyelinating myelopathies) • and • where necessary, institute prophylactic treatment to prevent recurrence.
SPINAL CORD • Acute and subacute myelopathy occurs for numerous reasons and should always be considered a medicalemergency. • Unfortunately, the diagnosis of myelopathy is often missed at first, leading to missed opportunities for treatment.
SPINAL CORD • Any patient who reports, or is found to have a sensory level on exam should be evaluated as a potentialmyelopathy patient. Also, patients who present with urinary retention should be considered a spinal corddysfunction patient until proven otherwise. • Patients with either a new sensory level or urinary retention should notbe discharged from an office or ER to home without complete imaging of the spinal cord with MRI.
SPINAL CORD AND ROOT COMPRESSION • CAUSES: -TUMOURS (PRIMARY, SECONDARY) EXTRADURAL, INTRADURAL, INTRAMEDULLARY • INFECTIONS (ACUTE, CHRONIC) • DISC DISEASE AND SPONDYLOSIS • HAEMATOMA (AVM, SPONTANEOUS, TRAUMA) - CYSTIC LESIONS (EXTRADURAL, INTRADURAL, INTRAMEDULLARY)
SPINAL CORD AND ROOT COMPRESSION • LEVEL OF THE LESION: • A lesion above the L1 vertebral body may damage both the cord and its roots. • Below this, only roots are damaged.
Categories of non-compressive acute myelopathies • Disorders that present as acute myelopathy can be grouped as follows: • 1. Vascular • 2. Demyelinating • 3. Infectious • 4. Non-infectious inflammatory • 5. Cancer related
LOCALIZING A PROCESS AT A SPECIFIC LEVEL IN THE SPINAL CORD • Foramen magnum and upper cervical cord: suboccipital pain and neck stiffness, Lhermitte’s symptom, occipital and finger tip paresthesias, syringomyelic-type sensory dissociation, spastic tetraparesis, long tract sensory signs, bladder disturbance,
APPROACH TO MYELOPATHIES WITH A NORMAL MRI • Has a compression been missed? (Epidural lipomatosis, Dynamic compression (flexion-extension studies) • • Is it really a myelopathy? (CNS: parasagittal meningioma, venous sinus thrombosis, ACA thrombosis, hydrocephalus, vascular parkinsonism, other EP disorders/ Ganglionopathy: Sjogren’s , B6, paraneoplastic/ • Plexopathy: paraneoplastic/ PNS: AIDP, NMJn: MG or LEMS, Muscle: periodic paralysis/ Motor neuronopathy: ALS/ PLS
APPROACH TO MYELOPATHIES WITH A NORMAL MRI • • Is it a metabolic/ toxic/ degenerative/ infective myelopathy? • • Are the images of adequate quality? (Include contrast?) • • Were the images taken too early or too late? • • Is the lesion too small to be seen on MRI? • • Is there subtle focal or generalized cord atrophy?
APPROACH TO MYELOPATHIES WITH A NORMAL MRI • • Is there a history of radiation?, Is there evidence of CSF hypovolemia?, • Is there evidence of superficial siderosis? • • Is it functional?
SPINAL CORD-SYNDROMES • Clinical presentation of spinal cord disorders: • The differential diagnosis of an acute myelopathy is dictated by the clinical setting in which the myelopathyoccurs, by the specific spinal syndrome, • the occurrence of systemic/non-neurological symptoms, • Radiographicappearance, • Clinical and radiological response to cortico-steroid therapy
SPINAL CORD-SYNDROMES • Spinal cord disorders are conventionally classified as ‘syndromes’ due to the typical signs and symptoms produced as a result of the location of lesions and tract involvement.
SPINAL CORD-SYNDROMES • For example, Brown-Séquard hemi cord syndrome indicates astructural myelopathy, either compressive or inflammatory and less often neoplastic disorders; it would be rarely • seen in vascular, paraneoplastic and metabolic disorders. In contrast, myelopathies with selective tract • involvement are characteristic of metabolic, paraneoplastic and degenerative myelopathies, rather than • inflammatory or infectious; for example, corticospinal and posterior columns involvement is typical of B12 and
SPINAL CORD-SYNDROMES • In contrast, myelopathies with selective tract involvement are characteristic of metabolic, paraneoplastic and degenerative myelopathies, rather thaninflammatory or infectious; for example, corticospinal and posterior columns involvement is typical of B12 and copper deficiency, adrenomyeloneuropathy, Friedreich’s ataxia.
SPINAL CORD-SYNDROMES • Complete spinal cord syndrome: • Description: Bilateral involvement of all tracts • Causes: Myelitis (parainfectious/ postvaccinal/ “transverse”), NMO, compression (trauma, tumor, hematoma,abscess), vascular, (rare with MS)
SPINAL CORD-SYNDROMES • Brown-Sequard syndrome (often incomplete): • Description: Pain and temperature loss contralateral to weakness, ipsilateral spastic weakness and loss ofproprioceptive function • Causes: compression or intrinsic cord lesion like demyelination
SPINAL CORD-SYNDROMES • Central cord syndrome: • Description: suspended analgesia, sacral sparing, dissociation of sensory loss, ipsilateral Horner, anteriorhorn dysfunction • Causes: syrinx, intramedullary tumors, hyperextension neck injuries (“man-in-a-barrel”)
SPINAL CORD-SYNDROMES • Posterolateral column disease: • Description: foot > hand paresthesias, dorsal column dysfunction, intact pain and temperature, corticospinaldysfunction, associated PN • Causes: Cbl/ copper deficiency, HTLV or HIV, extrinsic compression as in spondylotic myelopathy
SPINAL CORD-SYNDROMES • Posterior column disease: • Description: sensory ataxia, absent reflexes, hypotonic but not weak, hyperextensible joints, trophic changes,crises, decreased deep pain, Lhermitte’s • Causes: Tabes
SPINAL CORD-SYNDROMES • Anterior horn cell syndrome: • Description: weakness, atrophy, fasciculations, reduced tone and reflexes, intact sensations, possibleinvolvement of cranial motor nuclei • Causes: spinal muscular atrophy (infantile/ Werdnig-Hoffman, intermediate, juvenile-Kugelberg-Welander, motor neuron disease)
SPINAL CORD-SYNDROMES • Combined anterior horn cell and pyramidal tract disease: • Description: anterior horn cells and pyramidal tract, sphincteric sparing, asymmetric, cramping, bulbar or pseudobulbar involvement, sensory sparing, preserved superficial abdominals, reflexes variable, rare for extraocular muscles to be involved • Causes: ALS
SPINAL CORD-SYNDROMES • Anterior spinal artery syndrome: • Description: Bilateral corticospinal and spinothalamic involvement without dorsal column, bladder • dysfunction • Causes: Anterior spinal artery infarct or MS
SPINAL CORD-SYNDROMES • Posterior spinal artery syndrome; • Description: posterior column dysfunction with loss of segmental reflexes, infarction of unilateral posterior • horn and lateral column with sparing of posterior columns may also occur • Causes: posterior spinal artery infarct