Download
1 / 1
10 likes | 246 Views
Underlying Disorder. SUCCESSFUL MANAGEMENT OF OBSTETRICAL TEARS USING TOPICAL OXIDIZED REGENERATED CELLULOSE (SURGICEL ® ) IN DISSEMINATED INTRAVASCULAR COAGULAPATHY. Systemic Activation of Coagulation. Consumption Of Platelets And Clotting Factors. Widespread Intravascular Fibrin Deposition.

E N D
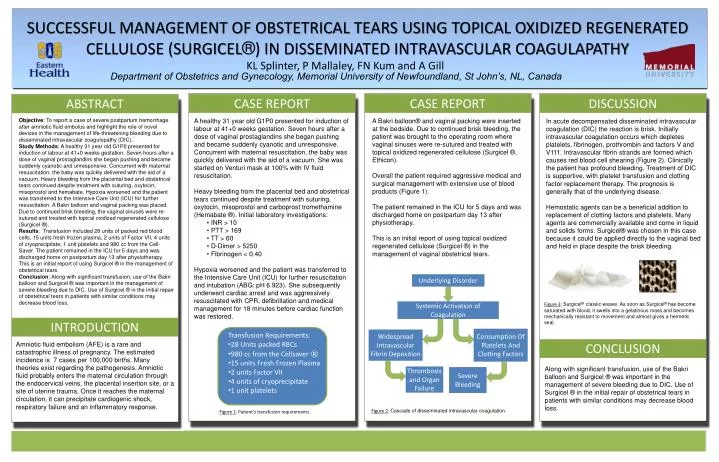
Underlying Disorder SUCCESSFUL MANAGEMENT OF OBSTETRICAL TEARS USING TOPICAL OXIDIZED REGENERATED CELLULOSE (SURGICEL®) IN DISSEMINATED INTRAVASCULAR COAGULAPATHY Systemic Activation of Coagulation Consumption Of Platelets And Clotting Factors Widespread Intravascular Fibrin Deposition KL Splinter, P Mallaley, FN Kum and A Gill Thrombosis and Organ Failure Severe Bleeding Department of Obstetrics and Gynecology, Memorial University of Newfoundland, St John’s, NL, Canada s CASE REPORT CASE REPORT DISCUSSION ABSTRACT Objective: To report a case of severe postpartum hemorrhage after amniotic fluid embolus and highlight the role of novel devices in the management of life-threatening bleeding due to disseminated intravascular coagulopathy (DIC). Study Methods: A healthy 31 year old G1P0 presented for induction of labour at 41+0 weeks gestation. Seven hours after a dose of vaginal prostaglandins she began pushing and became suddenly cyanotic and unresponsive. Concurrent with maternal resuscitation, the baby was quickly delivered with the aid of a vacuum. Heavy bleeding from the placental bed and obstetrical tears continued despite treatment with suturing, oxytocin, misoprostol and hemabate. Hypoxia worsened and the patient was transferred to the Intensive Care Unit (ICU) for further resuscitation. A Bakri balloon and vaginal packing was placed. Due to continued brisk bleeding, the vaginal sinuses were re-sutured and treated with topical oxidized regenerated cellulose (Surgicel ®). Results: Transfusion included 28 units of packed red blood cells, 15 units fresh frozen plasma, 2 units of Factor VII, 4 units of cryoprecipitate, 1 unit platelets and 980 cc from the Cell-Saver. The patient remained in the ICU for 5 days and was discharged home on postpartum day 13 after physiotherapy. This is an initial report of using Surgicel ® in the management of obstetrical tears. Conclusion: Along with significant transfusion, use of the Bakri balloon and Surgicel ® was important in the management of severe bleeding due to DIC. Use of Surgicel ® in the initial repair of obstetrical tears in patients with similar conditions may decrease blood loss. • A healthy 31 year old G1P0 presented for induction of labour at 41+0 weeks gestation. Seven hours after a dose of vaginal prostaglandins she began pushing and became suddenly cyanotic and unresponsive. Concurrent with maternal resuscitation, the baby was quickly delivered with the aid of a vacuum. She was started on Venturi mask at 100% with IV fluid resuscitation. • Heavy bleeding from the placental bed and obstetrical tears continued despite treatment with suturing, oxytocin, misoprostol and carboprosttromethamine (Hemabate ®). Initial laboratory investigations: • INR > 10 • PTT > 169 • TT > 60 • D-Dimer > 5250 • Fibrinogen < 0.40 • Hypoxia worsened and the patient was transferred to the Intensive Care Unit (ICU) for further resuscitation and intubation (ABG: pH 6.923). She subsequently underwent cardiac arrest and was aggressively resuscitated with CPR, defibrillation and medical management for 18 minutes before cardiac function was restored. A Bakri balloon® and vaginal packing were inserted at the bedside. Due to continued brisk bleeding, the patient was brought to the operating room where vaginal sinuses were re-sutured and treated with topical oxidized regenerated cellulose (Surgicel ®, Ethicon). Overall the patient required aggressive medical and surgical management with extensive use of blood products (Figure 1). The patient remained in the ICU for 5 days and was discharged home on postpartum day 13 after physiotherapy. This is an initial report of using topical oxidized regenerated cellulose (Surgicel ®) in the management of vaginal obstetrical tears. In acute decompensated disseminated intravascular coagulation (DIC) the reaction is brisk. Initially intravascular coagulation occurs which depletes platelets, fibrinogen, prothrombin and factors V and V111. Intravascular fibrin strands are formed which causes red blood cell shearing (Figure 2). Clinically the patient has profound bleeding. Treatment of DIC is supportive, with platelet transfusion and clotting factor replacement therapy. The prognosis is generally that of the underlying disease. Hemostatic agents can be a beneficial addition to replacement of clotting factors and platelets. Many agents are commercially available and come in liquid and solids forms. Surgicel® was chosen in this case because it could be applied directly to the vaginal bed and held in place despite the brisk bleeding. Ffff fffff Figure 3: Surgicel® classic weave. As soon as Surgicel® has become saturated with blood, it swells into a gelatinous mass and becomes mechanically resistant to movement and almost gives a hermetic seal. INTRODUCTION • Transfusion Requirements: • 28 Units packed RBCs • 980 cc from the Cellsaver ® • 15 units Fresh Frozen Plasma • 2 units Factor VII • 4 units of cryoprecipitate • 1 unit platelets Amniotic fluid embolism (AFE) is a rare and catastrophic illness of pregnancy. The estimated incidence is 7 cases per 100,000 births. Many theories exist regarding the pathogenesis. Amniotic fluid probably enters the maternal circulation through the endocervical veins, the placental insertion site, or a site of uterine trauma. Once it reaches the maternal circulation, it can precipitate cardiogenic shock, respiratory failure and an inflammatory response. CONCLUSION Along with significant transfusion, use of the Bakri balloon and Surgicel ® was important in the management of severe bleeding due to DIC. Use of Surgicel ® in the initial repair of obstetrical tears in patients with similar conditions may decrease blood loss. Figure 2: Cascade of disseminated intravascular coagulation. Figure 1: Patient’s transfusion requirements.