Download
1 / 24
480 likes | 1.27k Views
Cognitive Ergonomics. Prepared By : - Satyam Garg (0722913041) Nikhil Chaudhary (0722913023) Vibhu Agarwal (0722913055).

E N D
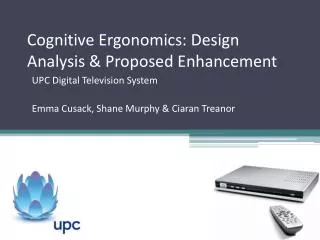
Cognitive Ergonomics Prepared By: - Satyam Garg (0722913041) Nikhil Chaudhary(0722913023) VibhuAgarwal(0722913055)
Cognitive ergonomics studies cognition in work settings, in order to optimize human well-being and system performance. It is a subset of the larger field of human factors and ergonomics. E. R. Vaidogas, Lectures on OSH
The definition of the field Ergonomics = human engineering = human factors Ergonomics = the science of fitting the job to the worker A multidisciplinary science that seeks to conform the workplace and all of its physiological aspects to the worker E. R. Vaidogas, Lectures on OSH
Domains of ergonomics International Ergonomics Association: Physical ergonomics human anatomical, anthropometric, physiological and biomechanical characteristics as they relate to physical activity (working postures, materials handling, repetitive movements, work related musculoskeletal disorders, workplace layout, safety and health.) Cognitive ergonomics: mental processes such as perception, memory, reasoning, and motor response, as they affect interactions among humans and other elements of a system (mental workload, decision-making, skilled performance, human-computer interaction, human reliability, work stress and training as these may relate to human-system design.) Organizational ergonomics: the optimization of sociotechnical systems including their organizational structures, policies, and processes (communication, crew resource management, work design, design of working times, teamwork, participatory design, community ergonomics, cooperative work, new work paradigms, virtual organizations, telework, and quality management.) E. R. Vaidogas, Lectures on OSH
The “role” of ergonomics in OSH Prevention of injuries and diseases E. R. Vaidogas, Lectures on OSH
The “traditional” application Workplace design and work organisation E. R. Vaidogas, Lectures on OSH
Muscular-skeletal disorders (MSDs) Work related heath problems by diagnosis group (EU-15, 1999) E. R. Vaidogas, Lectures on OSH
Economic costs of MSDs The situation in Europe • Although precise figures do not exist, estimates from Member States of the economic costs of all work related ill-health range from 2,6 to 3,8% of GDP. • A high proportion - maybe up to 40-50% - of the costs will be for musculoskeletal disorders. • Available cost estimates of MSD put the cost at between 0,5% and 2% of GDP. • More than 600 million working days are lost due to work related ill-health each year in Europe. • The costs to European business include: lost production; staff sickness, compensation and insurance costs; losing experienced staff and costs of recruiting and training new ones; effect of discomfort or ill health on the quality of work of employees. E. R. Vaidogas, Lectures on OSH
Dealing with MSDs 1/10 What is MSD? An “umbrella term” Work-related MSDs areimpairments of bodily structures(muscles, joints, tendons, ligaments, nerves, bones, and the localised blood circulation system), which are caused or aggravated primarily by work and by effects of work environment. Most MSDs arecumulative disorders, resulting from repeated exposure to high or low intensity loads over a long period of time. However, MSDs can also beacute traumas, such as fractures, which occur during an accident. E. R. Vaidogas, Lectures on OSH
Dealing with MSDs 2/10 Factors contributing to the development of MSDs (1/3) • Physical factors: • Force application, e.g. lifting, carrying, pulling, pushing, use of tools • Repetition of movements • Awkward and static postures, e.g. with hands above shoulder level, or prolonged standing and sitting • Local compression of tools and surfaces • Vibration • Cold or excessive heat • Poor lighting, e.g. can cause an accident • High noise levels, e.g. causing the body to tense E. R. Vaidogas, Lectures on OSH
Dealing with MSDs 3/10 Factors contributing to the development of MSDs (2/3) • Organisational and psychosocial factors: • Demanding work, lack of control over the tasks performed, and low levels of autonomy • Low levels of job satisfaction • Repetitive, monotonous work, at a high pace • Lack of support from colleagues, supervisors and managers E. R. Vaidogas, Lectures on OSH
Dealing with MSDs 4/10 Factors contributing to the development of MSDs (3/3) • Individual factors: • Prior medical history • Physical capacity • Age • Obesity • Smoking E. R. Vaidogas, Lectures on OSH
Dealing with MSDs 5/10 European prevention approach • Avoid MSD risks & evaluate MSD risks which can not be avoided • Combat the MSD risks at source • Adapt the work to the individual, especially the design of workplaces, the choice of work equipment and the choice of working and production methods, with a view, in particular, to alleviating monotonous work and work at a predetermined work-rate and to reduce their effect on health • Adapt to technical progress • Replace the dangerous by the non-dangerous or less dangerous • Develop a coherent overall prevention policy which covers technology, organisation of work, working conditions, social relationships and the influence of factors related to the working environment • Give collective protective measures priority over individual protective measures • Give appropriate instructions to workers E. R. Vaidogas, Lectures on OSH
Dealing with MSDs 6/10 Example 1: solutions to manual handling risks Lifting cast parts before and after the introduction of lifting/tipping containers E. R. Vaidogas, Lectures on OSH
Dealing with MSDs 7/10 Example 2: work at a pharmaceutical plant Before and after adjustments were made to a workstation E. R. Vaidogas, Lectures on OSH
Dealing with MSDs 8/10 Example 3: operator at assembly line for transformers Before - working with raised arm and elevated shoulder After - automated conveyor of adjustable height E. R. Vaidogas, Lectures on OSH
Dealing with MSDs 9/10 Example 4: awkward work posture in construction A special device introduced to protect knees. The device also functions as a stool E. R. Vaidogas, Lectures on OSH
Dealing with MSDs 10/10 Example 5: manoeuvring trolley Altering the handle height on this trolley improves posture andreduces effort required to push it E. R. Vaidogas, Lectures on OSH
The “role” of ergonomics in OSH Prevention of accidents E. R. Vaidogas, Lectures on OSH
Control room ergonomics 1/3 The origin of the problem The control room at Västerås old power plant (around 1920) E. R. Vaidogas, Lectures on OSH
Control room ergonomics 2/3 Increasing amount of information E. R. Vaidogas, Lectures on OSH
Control room ergonomics 3/3 Concentrating the operator’s information Cube display wall E. R. Vaidogas, Lectures on OSH
To end of part eleven E. R. Vaidogas, Lectures on OSH