Download
1 / 69
730 likes | 770 Views
Learn about the basis of drugs on chemokines, their biological functions, history, association with inflammatory responses, impact on T and B cell maturation, disease relevance, and development of targeting drugs. Discover key research findings and clinical trials in the field.

E N D
Drugs basis on Chemokines Speaker: Cheng, Hsi Tsung Date : 2012/10/16
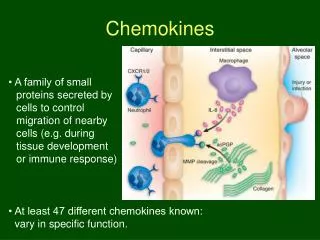
Chemokines • Chemoattractant Cytokines • Binding G protein-coupled receptors • 8-14 kDa
The origin and function of chemokines • The first member of the chemokine family to be discovered was platelet factor 4 • chemokines were not recognized as hemotactic molecules until the characterization of interleukin 8 • Association with inflammatory responses • Chemokines and receptors for T and B cell maturation
Chemokines and receptors for T and B cell maturation • Chemokines and their receptors control the movement of developing T and B cells • B cell chemokine receptors when disrupted, dramatically affects B cell hematopoiesis • Bone marrow spleen lymphoid tissue
Chemokines and receptors for T and B cell maturation • Medullary thymocytes, but not immature cortical thymocytes, respond to medullary stroma–expressed chemokines CCL19 and CCL21 (ligands for CCR7)
Chemokines and receptors for T and B cell maturation • Naïve T cells express receptors CXCR4 and CCR7 • Effector or memory T cells express CCR2, CCR3, CCR4, CCR5,CCR6, CCR8, CXCR5 and CCR9
+ELR: …ELRCXC…..C….…C.. CXC n>15 -ELR: ………CXC…..C….…C.. CC: n>25 …..CC…..C….…C…….. CX3C: n=1 …..CXXXC…..C….…C.. C: n=2 …..C…….…..C….….. Classification of Chemokines
Chemokine receptors and disease. multiple sclerosis, MS rheumatoid arthritis (RA) Inflammatory bowel disease (IBD)
Ligands • CXCL1,2,3,5,6,7,8 • Receptors • CXCR1 / CXCR2
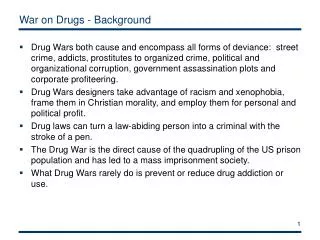
ELR+ CXC chemokines in pathology • Ulcerative colitis • Ischaemia/reperfusion injury • Tumor progression and spreading • Acute respiratory distress syndrome (ARDS) • COPD • Rheumatoid Arthritis
Antibodies • Abgenix obtained ABX-IL-8 • Filed the first Investigational New Drug (IND) in 1998 • Clinical trial for the therapeuticpotential in metastatic melanoma, psoriasis, rheumatoid arthritis(RA) and COPD • The clinical development was discontinued in 2002 (phase II) • Failed on psoriasis and RA
Antibodies • ABCream • Anti-CXCL8 monoclonal antibody • Penetrating through skin into psoriatic lesions. • Successfully completed in China Phase 4 • Clinical studies with ABCream in psoriatic patients. • official approval of production and marketing from the State Drug Administration (SDA) of China in 2001 and is currently marketed in China
Results of Phase III clinical trials in People's Republic of China (Phase IV trials complete as well) 49% to 53.8% of patientsachieved a greater than 60% improvement and 12.9% to 15.3% of patients achieved a greater than 90% improvement in PASI scores after a six week treatment cycle with ABCream.
GPCR Structure β2-adrenergic receptor
Mechanisms • CXCR1/2 Competitive antagonist • Allosteric inhibitor
Competitive antagonist • Since 1994 GlaxoSmithKline (GSK) has been running a program aimed at the development of small molecular weight CXCL8 antagonists. • SB225002 (1b (R1=NO2, R2=Br)) • In rabbits, 1b selectively inhibited CXCL8-mediated PMN margination • The efficacy of 1b was demonstrated in vitro and in vivo in different animal models but this molecule was not candidated to further development for undisclosed reasons.
Competitive antagonist • SB656933 • selected for clinical development and is currently undergoing Phase I clinical studies.
R1=NO2, R2=Br SB225002 SB656933
Competitive antagonist • Schering-Plough(Sch527123) • Completed Phase II clinical studies.
Allosteric inhibitor • Dompé pha.r.ma s.p.a. (reparixin) • undergoing Phase IIb clinical studies.
Receptor: CXCR1 Extra cellular domain Intra cellular domain (Leong et al.,JBC, 1994, 19343-48) Gray: CXCL8 binding<20% Black: CXCL8 binding<20% and Ca2+flux<10%
ECD peptide (Attwood et al, Bioorganic & Medicinal Chemistry Letters, 1996,1869-74)
ECD peptide (Attwood et al, Bioorganic & Medicinal Chemistry Letters, 1997, 429-32)
ECD peptide (Attwood et al, Bioorganic & Medicinal Chemistry Letters, 1997, 429-32)
CXCL8 • 72 residues • Produced by leukocytes and non-leukocyte somatic cells • Induced by inflammatory cytokines, bacterial, bacterial products, viral, environmental factors, tumor cell, etc. • expression level elevated in many inflammatory settings such as myocardial infarction (心肌梗塞), acute respiratory distress syndrome (ARDS) (呼吸窘迫症候群), COPD, and rheumatoid arthritis (類風濕性關節炎).
Receptors for CXCL8 (Brat et al.,Neuro-Oncology, 2005, 122-133) Kd 1 nM 1.2 nM 20 nM
CXCL8 mutants (Williams et al.,JBC, 1996, 9579-86) Clark-Lewis et al.,JBC, 1994, 16075-81)
CXCL8 mutants index=3 index=.85 index=3.1 index=6.5 (Williams et al.,JBC, 1996, 9579-86) Clark-Lewis et al.,JBC, 1994, 16075-81) Index= release fold / binding fold
Sequence Alignment The consensus of the various CXCL8 is 70%
hCXCL8(3-72)K11R/G31P (hG31P)An antagonist of CXCR1/2 blocked pleural hemorrhagic consolidation and neutrophil infiltration