Download
1 / 18
200 likes | 332 Views
Psychiatric illness in older people in general hospitals. John Holmes Senior Lecturer in Liaison Psychiatry of Old Age University of Leeds. Why bother about a problem?. If it is common If it affects outcomes. Older people are important. Two-thirds of general hospital beds High throughput

E N D
Psychiatric illness in older people in general hospitals John Holmes Senior Lecturer in Liaison Psychiatry of Old Age University of Leeds
Why bother about a problem? • If it is common • If it affects outcomes
Older people are important • Two-thirds of general hospital beds • High throughput • 20,000 non-scheduled admissions to LTHT • Leeds population 750,000 • 110,000 aged 65 years or over
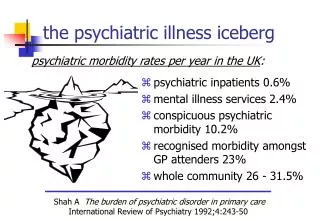
How common is psychiatric illness in older people in general hospitals?
So… • It’s common • But is it bad for you? • Outcomes of interest: • Mortality • Length of stay • Institutionalisation • Persistent symptoms • Resulting in: • Poorer quality of life • Or no life at all
…and if you have delirium J. Holmes and A. House. Psychiatric illness predicts poor outcome after surgery for hip fracture: a prospective cohort study. Psychological Medicine 30:921-929, 2000.
And as for survival… S. Nightingale, J. Holmes, J. Mason, and A. House. Psychiatric illness and mortality after hip fracture. Lancet 357 (9264):1264-1265, 2001
Why? • Psychiatric illness is not recognised • 50% of delirium • Psychiatric illness is not treated when recognised • Treatability • Knowing about and delivering the right treatment
But… • The NSF calls for the right skill-mix to meet the need in general hospitals • Though psychiatric staff are not routinely found there… • …and general hospital staff do not have the knowledge, skills and attitudes
The response of old age psychiatry? • Community focused • CMHTs, day hospitals, clinics • Psychiatric wards (some general hospital based) • Increasingly community based
Although… • 25% to 33% of all old age psychiatry referrals from general hospitals • Diagnosis, investigation, treatment of mental illness • Assess capacity • Arrange follow-up • Take over – take away
And… • Increased numbers of referrals • Pressure on acute beds • Changing patterns of reason for referral • More ill, older, frailer people in hospital • External influences (e.g. social services) • Concerns over consent and capacity • Referral pattern doesn’t match morbidity • Several specialities under-represented
Initial response time (M-W U Test p<0.0001)
Current response time M-W U-test p=0.012