Download
1 / 29
300 likes | 899 Views
Polymyalgia Rheumatica and Giant Cell Arteritis. Definition of Fibromyalga. “Chronic and widespread pain located at 11 or more of 18 tender points”-ACR definition No specific diagnostic test and no cure. Clinical manifestations. Chronic and persistent pain with varying manifestations

E N D
Definition of Fibromyalga • “Chronic and widespread pain located at 11 or more of 18 tender points”-ACR definition • No specific diagnostic test and no cure.
Clinical manifestations • Chronic and persistent pain with varying manifestations • Diffuse musculoskeletal pain, stiffness and fatigue • Joints not swollen painful or red • Sensation such as tingling, numbness, burning, crawling are often described • Pain is aggravated by change in weather, stress, fatigue, lack of sleep et cetera et cetera
Epidemiology • 2% of all US citizens affected: 5.5 million • Most common cause of generalized pain in women ages 20 to 50 • Prevalence increases with age: 2% ages 20 to 35, with 8% at age 70 • Females 10 times more common than males
Source: “The Manual Tender Point Survey”, D. Sinclair, T. Starz, D. Turk Univ. of Pittsburgh, School of Medicine
Tender points • Usually described with a number of kilos of pressure • In reality no real guidelines • 11 of 18 tender points • Fraught with controversy
: Comorbid conditions • Irritable bowel syndrome • Chronic fatigue syndrome • Migraine headache syndrome • Sleep disorder • Altered cognitive function • TM problems
Differential diagnosis • Polymyalgia rheumatica • Dermato or polymyositis • Hypothyroidism • Rheumatoid arthritis • Lyme disease • Toxic myopathies secondary to statin exposure or fibric acid
Definitions Polymyalgia Rheumatica (PMR) – Inflammatory condition of unknown etiology. Giant Cell Arteritis (GCA) – Vasculitis of medium or large arteries of unknown cause They often occur together so are suspected to have the same underlying pathophysiology.
PMR • Diagnosis is difficult and uncertain as the symptoms are non-specific. As such incidence is hard to predict. • Shoulder and/or pelvic girdle pain with early morning stiffness forms the polymyalgic syndrome. • There is no diagnostic test and is in many ways a diagnosis of exclusion.
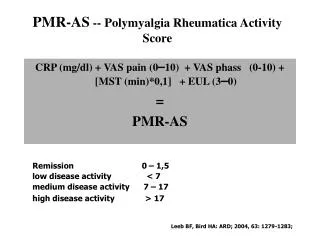
Bird Criteria (3 or more) • Bilateral shoulder pain or stiffness • Onset of illness less than 2 weeks • Initial ESR >40 • Morning stiffness >1hr • Age 65 or older • Depression and/or weight loss • Bilateral tenderness in upper arms
PMR • Take care not to miss other causes of the symptoms • PMR less likely to be the cause if: incomplete response to steroids, muscular weakness, prominent peripheral joint symptoms, lack of morning stiffness, unilateral symptoms. • ESR/CRP are usually raised, normochromic normocytic anaemia is common, LFT’s esp AlkP may be abnormal.
PMR • It’s complications are debility due to pain. • 20% will develop GCA • Response to steroid is rapid though some patients are hard to wean off steroids.
GCA • 3 times more common in females • Also known as temporal arteritis • Affects cranial branches of arteries from arch of aorta and branches of ophthalmic artery. • Associated with critical ischaemia : stroke blindness. • These can occur very early in the disease.
GCA • Rare if <50y old • Unilateral headache most often in temporal region. • Scalp tenderness classically noticed while brushing hair. • Pain on chewing – claudication of muscles of mastication • Fever, weight loss, fatigue, anorexia.
GCA • Double vision or amaurosis fugax (transient painless loss of monocular vision of variable duration) • Can have reduced visual acuity and/or visual field defects. • Fundoscopy – oedema/pallor of optic disc small retinal haemorrhages may also be seen
GCA • Include general CV examination – check BP both arms as aortic dissection can occur. • Check peripheral pulses and listen for carotid bruits. • The American College Of Rheumatology (ACR) is a helpful diagnostic criteria.
ACR Criteria for GCA(three or more needed) • Age 50 or greater • New type of headache • Clinically abnormal temporal artery (thickened, tender or nodular decreased pulsation) • ESR 50 or > • Abnormal artery biopsy – necrotizing arteritis with mononuclear infiltrate or granulomatous infiltrate usually with multinucleated giant cells!
GCA • Inflammatory markers are not always raised do not withhold treatment if strong clinical suspicion. • As PMR normochromic normocytic anaemia is common as are abnormal LFT’s • Use of temporal artery biopsy is debated - + confirms GCA but negative does not exclude due to skip lesions
GCA • Large artery complications common • Aortic aneurysm or dissection occurs in 18%!!! • Patients with GCA have a higher risk of stroke/MI/CHF. • A variety of neurological complications can also ensue • Early adequate dose steroids prevent most complications.
Headache Scalp tenderness Thickened temporal arteries Jaw claudication Acute visual loss Weight loss, anorexia, fever, night sweats, malaise & depression GIANT CELL ARTERITISPresentation
GIANT CELL ARTERITIS Temporal Artery Biopsy • Arteries have skip lesions • ultrasound/Doppler may help identify involved areas • If positive, confirms diagnosis – helpful in management of future disease • If negative, doesn’t exclude diagnosis, but need to think about an alternative diagnosis
Management of PMR and GCA • Follows pattern of induction, maintenance and reduction of treatment. • Most evidence for steroid dose is observational • Oral prednisolone is the most common treatment used.
Management of PMR and GCA • PMR no signs GCA • Prednisolone 10-20mg od (after baseline investigations) • 70% improve in 1/52 • Inflammatory markers improve in 3-4/52 2) GCA without visual disturbance • 40-60mg prednisolone od • R/V at 48hrs sooner if visual disturbance
Management of PMR and GCA 3) GCA with visual disturbance - Medical emergency 60mg prednisolone urgent admission to ophthalmologists
Maintenance • PMR and GCA continue dose steroid for up to 4 weeks then can be decreased every 2-4weeks 5mg a time in GCA and 2.5mg in PMR. • When on 10mg decrease every 4-6weeks by 1mg • When on 7mg maintain at this for 12months before reducing further. • Steroids should only be stopped if proximal pain and morning stiffness have resolved. • Helpful to monitor CRP/ESR during above • Can relapse requiring step up in steroid again
Who and when to Refer? • GCA any with visual symptoms even if on treatment should be referred on that day to ophthalmology. • Other patients with GCA – routine referral to rheumatology or general medicine for shared care. • PMR can be managed in GP setting • Consider secondary care referral if doubt as to diagnosis, poor response to treatment or adverse effects with steroid treatment.
Considerations • Don’t forget long term risks of steroid treatment especially if used for 12-24+months • Frequent BP and bloods should be offered • Osteoporos is important consideration • Encourage increased activity
Summary • PMR – pain+stiffness proximal muscles GCA vasculitis – headaches/scalp tenderness • GCA vasculitis – headaches/scalp tenderness • GCA can cause irreversible blindness • ESR + CRP are commonly raised in GCA +PMR • Dramatic response to corticosteroids in both • Relapse common during steroid reduction • Patients require long term steroids thus use osteoporosis prophylaxis as per local guidelines.