Download

1 / 29
290 likes | 359 Views
Associations Between Outpatient Heart Failure Process of Care Measures and Mortality.

E N D
Associations Between Outpatient Heart Failure Process of Care Measures and Mortality Gregg C. Fonarow, Nancy M. Albert, Anne B. Curtis, Mihai Gheorghiade, J. Thomas Heywood, Mark L. McBride, Patches Johnson Inge, Mandeep R. Mehra, Christopher M. O'Connor, Dwight Reynolds, Mary N. Walsh,Clyde W. Yancy Fonarow GC, et al. Circulation. 2011;123(15):1601-1610.
Disclosures The IMPROVE HF registry is sponsored by Medtronic The sponsor had no role or input into the selection of endpoints or quality measures used in the study Outcome Sciences, Inc, a contract research organization, independently performed the practice site chart abstractions for IMPROVE HF, stored the data, and provided benchmarked quality of care reports to practice sites. Outcome Sciences received funding from Medtronic. Individually identifiable practice site data were not shared with either the steering committee or the sponsor Individual author disclosures are provided in the manuscript Fonarow GC, et al. Circulation. 2011;123(15):1601-1610.
Heart Failure Care in the Outpatient Cardiology Practice Setting There are well documented gaps, variations, and disparities in the use of evidence-based, guideline recommended therapies for heart failure (HF) in inpatient and outpatient care settings. IMPROVE HF showed a performance improvement program can increase the use of guideline recommended HF therapies in the outpatient setting. It is assumed that use of process based performance measures are associated with improved clinical outcomes; however that has not been evaluated for current or emerging outpatient HF measures. Fonarow GC, et al. Circulation. 2011;123(15):1601-1610.
IMPROVE HF Outpatient Process Measures Yancy CW, et al. Circulation. 2005;112:154-e235. Bonow RO, et al. J Am Coll Cardiol. 2005;46:1144-1178.
Study Objectives Fonarow GC, et al. Circulation. 2011;123(15):1601-1610.
Statistical Methods For primary analysis, patients who were eligible for treatment but not treated at baseline and who crossed over within first 12 months of the performance initiative were excluded from each measure The composite score for each patient was calculated as the sum of individual quality measure numerators divided by the sum of individual quality measure denominators for which patient was eligible The all-or-none care measure was defined for each patient in terms of whether they received all individual measures for which they were eligible Process-of-care measure conformity at baseline stratified by vital status at 24 months was summarized andcompared in patients alive vs. those who died by Chi-square test or t test For each quality measure, composite score and all-or-none care measure, Generalized Estimating Equation (GEE) methodology was used to estimate unadjusted and adjusted relationships between each process measure and patient-level mortality in first 24 months. The GEE models accounted for correlation of patients within practices. Appropriate clinical and/or statistical meaningful baseline patient demographic and clinical characteristics and practice characteristics were included in the multivariate GEE model for adjusted odds ratio estimation Fonarow GC, et al. Circulation. 2011;123(15):1601-1610.
Patient Population • To be enrolled in IMPROVE HF, patients had to have heart failure or post-myocardial infarction left ventricular dysfunction with left ventricular ejection fraction of 35% or less. • There were 15,177 patients from 167 cardiology and multispecialty practices in the US evaluated at baseline and enrolled in the longitudinal cohort. • At the 24 month follow-up 11,621 of the 15,177 patients (76.6%) had documentation of vital status. • A total of 2507 patients (16.5%) were lost to follow-up and 1048 (6.9%) were seen in practices (n=12) that did not complete the follow-up assessment. Fonarow GC, et al. Circulation. 2011;123(15):1601-1610.
IMPROVE HF Patient Characteristics Fonarow GC, et al. Circulation. 2011;123(15):1601-1610.
Patient Characteristics (Continued) Fonarow GC, et al. Circulation. 2011;123(15):1601-1610.
IMPROVE HF Practice Characteristics Fonarow GC, et al. Circulation. 2011;123(15):1601-1610.
Patient 24 Month Follow-up Mortality • At 24 months, 2569 of the 11,621 patients (22.1%) with complete vital status had died. • Patients who died were significantly more likely to have ischemic HF origin and comorbidities, including diabetes mellitus, hypertension, chronic obstructive pulmonary disease, peripheral vascular disease, and depression. • Statistically significant differences were also evident for laboratory evaluations, including BUN and creatinine, with higher levels in patients who had died during the 24-month follow-up. • The baseline process measure conformity was significantly lower among patients who died compared with those who survived for 5 of the 7 individual measures. Fonarow GC, et al. Circulation. 2011;123(15):1601-1610.
Baseline Measure Conformity: Alive vs. Dead at 24-Month Follow-Up The baseline process measure conformity was significantly lower among patients who died compared with those who survived for 5 of 7 individual measures. Fonarow GC, et al. Circulation. 2011;123(15):1601-1610.
Association Between HF Process Measures and Mortality: Univariate and Multivariate GEE Models Fonarow GC, et al. Circulation. 2011;123(15):1601-1610.
6 of 7 Process Measures Associated with Reduced Mortality Mortality Adjusted Odds Ratios with 95% CI Displayed Fonarow GC, et al. Circulation. 2011;123(15):1601-1610.
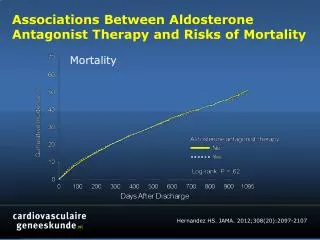
Composite Measures Associated with Reduced 24 Month Mortality • Each 10% improvement in composite care was associated with a 13% lower odds of 24-month mortality (adjusted odds ratio, 0.87; 95% confidence interval, 0.84 to 0.90; P<0.0001). • The adjusted odds for mortality risk for patients with conformity to each measure for which they were eligible was 38% lower than for those whose care did not conform for 1 or more measures for which they were eligible (adjusted odds ratio, 0.62; 95% confidence interval, 0.52 to 0.75; P<0.0001). Fonarow GC, et al. Circulation. 2011;123(15):1601-1610.
Results Summary Baseline process measure conformity was significantly lower among patients who died compared to those who survived for 5 of 7 measures (ACEI/ARB, beta-blockers, anticoagulation for atrial fibrillation, ICD, CRT). Baseline process measure composite score was 70.0% for patients alive at 24 months compared to 63.4% for those who died (p <0.0001). Adjusted odds ratio for mortality risk for patients with conformity to all eligible measures was 38% lower than those without conformity to one or more eligible measure. Every 10% improvement in composite care was associated with a 13% lower odds of 24 month mortality risk. Fonarow GC, et al. Circulation. 2011;123(15):1601-1610.
Study Limitations Patient eligibility and utilization rates were determined by accuracy and completeness of medical records and their abstraction Reasons for preventing treatment may not have been documented NYHA was not quantified in many records and instead was based on qualitative description of the patient’s functional status Potential for ascertainment bias Self-selected cardiology practices, primary care setting not included Not randomized – secular trends may have influenced results Follow-up not available for all patients Study analyzed medications prescribed rather than patient adherence Associations between care processes and outcomes do not determine causality Did not assess health-related quality of life, symptom control, functional capacity, patient satisfaction, hospitalization rates, or other clinical outcomes that may be of interest Fonarow GC, et al. Circulation. 2011;123(15):1601-1610.
Conclusions These data are among the first to demonstrate that adherence to HF process measures for ACEI/ARB, beta blocker, anticoagulation for atrial fibrillation, and HF education is significantly associated with survival in outpatients with heart failure. Process measures for ICD use and CRT use could also be considered for inclusion in HF outpatient performance measure sets. Fonarow GC, et al. Circulation. 2011;123(15):1601-1610.
Clinical Implications These HF process measures appear to discriminate the quality of HF care at the patient level and may be useful for assessing and improving HF care. Fonarow GC, et al. Circulation. 2011;123(15):1601-1610.
IMPROVE HF Study Overview • Largest, most comprehensive performance improvement study for HF patients in the outpatient setting • Designed to enhance quality of care of HF patients by facilitating adoption of evidence-based, guideline-recommended therapies: • Evaluate utilization rates of evidence-based, guideline-recommendedHF therapies at baseline and over the course of the performance improvement intervention (chart audit and feedback; use of performance measures) • Multifaceted, practice-specific performance improvement toolkit including clinical decision support tools (reminder systems) • Sites attended an educational workshop to set treatment goals and develop a customized clinical care pathway (educational outreach) Fonarow GC, et al. Am Heart J. 2007;154:12-38.
Methods: Guideline-Recommended Quality Measures Seven quality measures with strong evidence prospectively selected: Angiotensin-converting enzyme inhibitor (ACEI) or angiotensin II receptor blocker (ARB)* ß-blocker* Aldosterone antagonist Anticoagulation therapy for atrial fibrillation/flutter (AF)* Cardiac resynchronization therapy with or without ICD (CRT) Implantable cardioverter defibrillator with or without CRT (ICD) Heart failure (HF) education* Patients deemed eligible for individual quality measure based on meeting guideline criteria, without contraindications, intolerance, or other documented reasons for non-treatment Steering committee selected quality measures based on potential to improve patient outcomes, definition precision, construct and content validity, feasibility * Included as ACC/AHA outpatient HF performance measure, endorsed by National Quality Forum. Fonarow GC, et al. Circulation. 2010;122:585-596.
Methods: Patient Selection, Practice Selection, Data Collection and Management Patient Inclusion: Clinical diagnosis of HF or prior MI with at least 2 prior clinic visits within 2 years LVEF ≤ 35% or moderate to severe left ventricular dysfunction Patient Exclusion: Cardiac transplantation Estimated survival < 1 year from non-cardiovascular condition Average of 90 eligible patients per practice randomly selected for each of 3 study cohorts Practices: Outpatient cardiology (single specialty or multi-specialty) practices from all regions of the country Data quality measures 34 trained, tested chart review specialists Training oversight by study steering committee members Monthly quality reports Automated data field range, format, unit checks Chart abstraction quality Interrater reliability averaged 0.82 (kappa statistic) Source documentation audit sample concordance rate range of 92.3% to 96.3% Coordinating center: Outcome Sciences, Inc. (Cambridge, MA) Individual practice data not shared with sponsor or steering committee Fonarow GC, et al. Circulation. 2010;122:585-596.
Methods: Study Design and Patient Disposition • Patients who were eligible for treatment but not treated at baseline and who crossed over within the first 12 months of the intervention were excluded from each measure Fonarow GC, et al. Circulation. 2010;122:585-596.
Methods: Practice Specific Performance Improvement Intervention Practice Survey: 96% adopted one or more performance improvement strategies 85% used benchmarked quality reports 60% employed one or more IMPROVE HF tools * Use or participation was encouraged but not mandatory. Practices could adopt or modify tools. Fonarow GC, et al. Circulation. 2010;122:585-596.
IMPROVE HF Performance Intervention:Benchmarked Practice Profile Report
IMPROVE HF Performance Improvement Tools As part of an enhanced treatment plan, IMPROVE HF provided evidence-based best-practices algorithms, clinical pathways, standardized encounter forms, checklists, pocket cards, chart stickers, and patient education and other materials to facilitate improved management of outpatients with HF The materials can be downloaded from www.improvehf.com The materials are also included in the Circulation online-only Data Supplement Fonarow GC, et al. Circulation. 2010;122:585-596.
IMPROVE HF Practice Specific Education and Implementation Tools Evidence Based Algorithms and Pocket Cards Clinical Trials and Current Guidelines Clinical Assessment and Management Forms www.improvehf.com Patient Education Materials • Dissemination of best practices: • Webcasts • Online Education • Newsletters