Download
1 / 10
100 likes | 114 Views
Payment Reform: Physician Perspectives Alliance for Health Reform Washington, DC March 20, 2009. Nancy H. Nielsen, MD, PhD President, American Medical Association. First Things First. AMA agrees with President Obama that health care reform is a high priority

E N D
Payment Reform:Physician Perspectives Alliance for Health Reform Washington, DC March 20, 2009 Nancy H. Nielsen, MD, PhDPresident, American Medical Association
First Things First • AMA agrees with President Obama that health care reform is a high priority • AMA meeting with top Administration officials & Congressional leaders, wants reform effort to succeed
Payment Reform Framework Physicians understand need for change; want reforms that improve coordination and quality of care, focus on prevention and reduce growth of health care costs Agree that different practices will have different capabilities to move toward bundling or pay based on performance Flexibility is needed to allow practices to adopt what works best for them Antitrust reform is needed to allow physicians to achieve desired integration
Payment Reform Framework • Specialty societies should be encouraged to help design innovative models using performance measures and appropriateness criteria • Health care data should be shared with physicians and medical societies to help them improve appropriateness and quality of care • Liability reform is also key to slowing growth in costs and improving appropriateness
Options for Reform • Further development and testing are needed of medical homes, gainsharing, accountable care organizations, pay-for-performance and bundled payments • Details matter, i.e., does money from bundled payments flow to hospital, or to physician-hospital organization? Can ACOs be set up without hospitals? • HIT adoption and comparative effectiveness research will compliment payment reform experiments • Don’t expect a “one size fits all” approach to payment reform
Incentives for Coordination and Quality • Need to provide incentives to all members of the patients’ care team so they coordinate with primary care physician • Patients with multiple chronic conditions need care coordinated with specialists, hospitalists and primary care • Make sure physicians have good information about what works and try to make gray areas less gray • Many factors drive variation, including patients’ preferences, socioeconomic status and religious beliefs • Expanding insurance coverage and encouraging healthy choices about food, exercise and tobacco use can help reduce variation
Incentives for Coordination and Quality • All physicians need better support for their efforts to improve care and reduce fragmentation • Paying for care coordination will provide better support for primary care physicians, but funding should not come from pay cuts for specialty care • Robbing Peter to pay Paul is likely to exacerbate workforce shortages and curtail patient access • Dividing medicine will make it difficult for physicians to unite behind efforts to reform the system
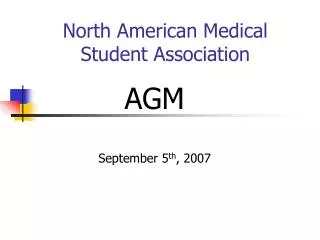
PHYSICIAN SHORTAGES ARE DEVELOPING 2025 Shortage = ~200,000 Physicians if demand grows at historical rates 2000 Demand Supply 1930 Source: R. Cooper, MD, Univ. of Pennsylvania
If not now, when? • Invest in prevention, care coordination, expanded coverage, HIT, comparative effectiveness research • Test new payment models and incentives • Support antitrust and liability reform • Enhance value-based decision making throughout the health care system