Download
1 / 67
780 likes | 1.01k Views
AUTOIMMUNE DISEASES. Department of Immunology and Allergology Faculty of Medicine and Faculty Hospital in Pilsen. AUTOIMMUNE DISEASES. chronic and usually irreversible incidence: 5% - 7% of population, higher frequencies in women, increases with age. Autoimmune disease s.

E N D
AUTOIMMUNE DISEASES Department ofImmunologyandAllergology FacultyofMedicineandFacultyHospital in Pilsen
AUTOIMMUNE DISEASES • chronic and usually irreversible • incidence: 5%-7% of population, higher frequencies in women, increases with age
Autoimmune diseases • Immunological tolerance is specific unresponsiveness to an antigen • Self tolerance - all individuals are tolerant of their own (self) antigens, thefundamentalcharacteristicoftheimmunesystem Autoimmunediseasses result from a failure of self- tolerance, immune response isactivatedagainst self antigens - causesdamageofowntissues.
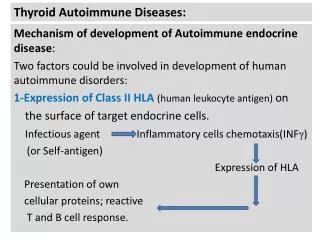
Autoimmunity • The principal factors in the development of autoimmunity are the inheritance of susceptibility genes and environmental triggers, such as infections • Most autoimmune diseases are polygenic and are asssociatedwith multiple gene loci, the most important of which are the MHC genes • Infections may activate self-reactive lymphocytes, thereby trigger the development of autoimmune diseases
AUTOIMMUNE PATOLOGICAL RESPONSE - ETIOLOGY Factors contributing to autoimmunity: - internal (HLA association, polymorphism of cytokine genes, defect in genes regulating apoptosis, polymorphism in genes for TCR and H immunoglobulin chains, association with immunodeficiency, hormonal factors) Internal triggering factors • genotype / HLA • cytokines • apoptosis genes • ID (IgA, CVID, C1,2,4), • hormones
AUTOIMMUNE PATOLOGICAL RESPONSE - ETIOLOGY Factors contributing to autoimmunity: - external (infection, stress by activation of neuroendocrinal axis and hormonal dysbalance, drug and ionization through modification of autoantigens) Externaltriggeringfactors • infections • UV • drugs • chemicals • stress
AUTOIMMUNE PATOLOGICAL RESPONSE - PATHOGENESIS • type II. by Coombs and Gel: cytotoxic immune reaction 1. damage of tissue 2. functional impact (stimulation, inhibition, neutralization) • type III. by Coombs and Gel: immune complex • type IV. by Coombs and Gel Mechanismoftissuedamage:
Type II immunopatologicalreaction • IgMand IgGAb promote the phagocytosis of cells which they bindormay interfere with the functions of cells (inhibit, stimulate) by binding to essential molecules and receptors. • Graves‘ disease, Pernicious anemia, Myasthenia gravis, Acute rheumatic fever, Goodpasture‘s syndrome, Pemphigusvulgaris, Autoimmune hemolytic anemia or thrombocytopenicpurpura
Type IIIimmunopatological reaction • Ab may bind to circulating antigens to form immune complexes, which deposit in vessels and cause tissue injury • Injury is mainlydue to leukocyte recruitment and inflammation • Systemic lupus erythematosus, Polyarteritisnodosa, Poststreptococcalglomerulonephritis
Type IV immunopatologicalreaction • T cell- mediateddiseases are caused by Th1-mediateddelayed-type hypersensitivityreactionsor Th17- mediatedinflammatoryreactions, or by killingof host cells by CD8+ CTLs (cytotoxiclymphocytes). • Diabetes mellitus (insulin-dependent), Rheumatoid arthritis, Multiple sclerosis, Inflammatoryboweldisease
Autoimmunediseases • Organ-specific organ specificautoantibodies orautoreactive T lymphocytes • Systemic organ non-specific autoantibodies • Organ-localised • non-specific autoantibodies
CLINICAL CATEGORIES • systemic - affect many organs and tissue - organ non-specificautoantibodies • organ specific - affect one organ - organ specificautoantibodiesorautoreactive T lymphocytes • organlocalised - affect predominantly one organ accompanied by affection of other organs (inflammatory bowel diseases, coeliac disease, AI hepatitis, pulmonary fibrosis) - organ non-specificautoantibodies
EXAMPLES OF SYSTEMIC AUTOIMMUNE DISEASES examples autoantibodies
SYSTEMIC AUTOIMMUNE DISEASES • Systemic lupus erythematosus • Rheumathoid arthritis • Sjögren‘s syndrome • Dermatopolymyositis • Systemic sclerosis • Mixed connective tissue disease • Vasculitis
SYSTEMIC LUPUS ERYTHEMATOSUS • chronic, inflammatory, multiorgan disorder • autoantibodies react with nuclear material and attack cell function, immune complexes with dsDNA deposit in the tissue • multiple tissuesare involved including the skin, mucosa, kidney, joints, brain and cardiovascular system • general symptoms: include malaise, fever, weight loss • characteristic signs: butterfly rash, renalmanifestation, CNS manifestation, pulmonary fibrosis
DIAGNOSTIC TESTS • an elevated ESR (erythrocyte sedimentation rate), low CRP, trombocytopenia, leucopenia, hemolytic anemia, decreased levels of complement compounds(C4, C3), elevated serum Ig levels, immune complexes in serum
AUTOANTIBODIES • Autoantibodies: ANA, dsDNA(double-stranded), ENA (SS-A/Ro, SS-B/La,Sm), against histones, phospholipids
SLE American College of Rheumatology criteria (4/11) Arthralgia Neurological abn Oral ulcers Haematological abn Serositis Renal disease Malar rash Anti-nuclear factor Discoid rash Immunological abn Photosensitivity
RHEUMATOID ARTHRITIS • chronic, inflammatory disease with systemic involvement • characterized by an inflammatory joint lesion in the synovial membrane, destruction of the cartilage and bone, results in the joint deformation • clinical features: arthritis, fever, fatigue, weakness, weight loss • systemic features: vasculitis, pericarditis, uveitis, nodules under skin, intersticial pulmonary fibrosis • diagnostic tests: - elevated CRP and ESR, elevated serum gammaglobulin levels - autoantibodiesagainst IgG = rheumatoid factor (RF), a-CCP (cyclic citrullinepeptid) - X-rays of hands and legs- show a periarticular porosis, marginal erosion
SJÖGREN‘S SYNDROME • chronic inflammatory disease affecting exocrine glands • the primary targetsare the lacrimal and salivary gland duct epithelium • general features: malaise, weakness, fever • Typicalclinicalfeatures: dry eyes and dry mouth, swollen salivary glands, dryness of the nose, larynx, bronchi and vaginal mucosa • primary syndrome • secondary syndrome – is associated with other AI diseases (SLE, RA, sclerodermia, polymyositis, primary biliarycirhosis,AIthyroiditis) • autoantibodies against ENA (SS-A, SS-B), ANA • The Schirmer test - measures the production of tears
Dermatopolymyositis • a connective-tissue disease characterized by inflammation • of the muscles and the skin. Gottron's sign is an erythematous, scaly eruption occurring in symmetric fashion over the MCP and interphalangeal joints Heliotrope rash is a violaceous eruption on the upper eyelids, often with swelling
Dermatopolymyositis • elevatedcreatinephosphokinase (CPK) • muscle biopsy (a mixed B- and T-cell perivascular inflammatory infiltrate, perifascicular muscle fiber atrophy) • EMG (electromyogram) • autoantibodies- ENA (Jo-1)
Systemic sclerosis • sclerosis in the skin or other organs • Diffuse scleroderma(progressive systemic sclerosis) is the most severe form, involves skin, will generally cause internal organ damage (specifically the lungs and gastrointestinal tract) • The limited formis much milder • The limited form is often referred to as CREST syndrome(CREST is an acronym for the five main features: Calcinosis, Raynaud's syndrome, Esophageal dysmotility, Sclerodactyly, Telangiectasia
Immunological findings • ANA, ENA - anti-Scl-70 (fluorescence of nucleolus)or anti-centromers
Mixed connective tissue disease • combines features of polymyositis, systemic lupus erythematosus, scleroderma, and dermatomyositis(overlap syndrome) • features : joint pain/swelling, malaise, Raynaud phenomenon, muscle inflammation and sclerodactyly (thickening of the skin of the pads of the fingers) • distinguishing laboratory characteristics: a positive, speckled anti-nuclear antibody (ANA) and anti-U1-RNP antibody (ENA)
Vasculitis • characterized by inflammatory destruction of vessels leading to thrombosis and aneurysms • affect mostly lung, kidneys, skin • Symptoms: fatigue, weakness, fever, arthralgias, abdominal pain, hypertension, renal insufficiency, neurologic dysfunction…
Vasculitis diagnostic tests: elevated ESR, CRP, leucocytosis, biopsy of affected organ (necrosis, granulomas), angiography, ANCA (antineutrophil cytoplasmic antibodies) • p- ANCA (myeloperoxidase) positivity (Polyarteritisnodosa, Churg- Strauss) • c- ANCA (serinproteinase) positivity(Wegener granulomatosis)
Clasificationofvasculitis • Takayasu • Giant cell (temporal) arteriitis • Polyarteritis nodosa • Churg-Strauss arteritis • Kawasaki disease • Henoch-Schönlein purpura • Wegener´s granulomatosis • Large vessel • Mediumandsmallvessel • Smallvessel
Autoimmunesystemicdiseases- characteristicautoantibodies • SLE ANA, dsDNA, ENA-Sm • Rheumatoid arthritis RF • Dermato/polymyositis ENA Jo-1 • Sjögren´s syndrome ENA SS-A, SS-B • Sklerodermia ENA Scl 70 • MCTD ENA RNP • Antiphospholip. syndrome anti-phospholipides • Vasculitis ANCA
EXAMPLES OF ORGAN LOCALISED AUTOIMMUNE DISEASES diseases autoantibodies
ORGAN LOCALIZED AUTOIMMUNE DISEASESLocalizedautoimmunediseaseswithsystemicautoantibodies • Ulcerative colitis • Crohn‘s disease • Autoimmune hepatitis • Primary biliarycirhosis • Pulmonary fibrosis
Ulcerative colitis • chronic inflammation of the large intestine mucosa and submucosa • features: diarrhea, bloody and mucusstools • extraintestinal features (arthritis, uveitis) • autoantibodiesagainst atypicalANCA (lactoferin, cathepsin…), a- large intestine
Crohn‘s disease • the granulomatous inflammation of wholeintestinal wall with ulceration and scarring that can result in abscess and fistula formation • the inflammation inCrohn's disease the most commonly affects the terminal ileum, presents with diarrhea and is accompanied by extraintestinal features - iridocyclitis, uveitis, artritis, spondylitis • antibodies againstSaccharomycescerevisiae (ASCA), a- pancreas
Primary biliarycirhosis autoimmune disease of the liver marked by the slow progressive destruction of the small bile ducts; can lead to cirrhosis AMA= antimitochondrialautoantibodies
AUTOIMMUNE HEPATITIS • typeI – association with autoantibodies against smooth muscles SMA • type II –autoantibodies against microsomesLKM-1 = liver-kidney microsomes • type III – autoantibodies against SLA (solubile liver antigen)
ORGAN SPECIFIC AUTOIMMUNE DISEASES • Autoimmune endocrinopathy • Autoimmune neurological diseases • Autoimmune cytopenia
AUTOIMMUNE ENDOCRINOPATHY • Hashimoto‘s thyroiditis • Graves-Basedow disease • Diabetes mellitus I. type • Addison‘s disease • Autoimmune polyglandular syndrome • Pernicious anemia
Hashimoto‘s thyroiditis • thyroid disease result to hypothyroidism on the base of lymphocytes and plasma cells infiltrate • autoantibodies against thyroidal peroxidase (a-TPO) and/or against thyroglobulin (a-TG)
infiltrate of plasma cells and lymphocytes with germinal center formation is seen in this thyroid
Grave‘s disease • thyrotoxicosis from overproduction of thyroid hormone (patient exhibit fatigue, nervousness, increased sweating, palpitations, weight loss, exophtalmus) • autoantibodies against thyrotropinreceptor, autoantibodies cause thyroid cells proliferation
Diabetes mellitus (insulin- dependent) • characterized by an inability to process sugars in the diet, due to a decrease in or total absence of insulin production • results from immunologic destruction of the insuline- producing β-cells of the islets of Langerhans in the pancreas • autoantibodies against GAD- glutamic acid decarboxylase = primary antigen), autoantibodies anti- islet cell, anti- insulin • islets are infiltrated with B and T cells
Polyglandular autoimmune syndrome • combination of several different AI endocrinopathies • autoantibodies appear in according with the connected disorders
Pernicious anemia • autoantibodies against parietal cells of gastric mucose, against intrinsic factor (transportation of B12 vitamin) • the deficiency of the intrinsic factor results in vitamin 12 malabsorptionwithabnormal formation of erythrocytes clinical feature- atrophic gastritis, macrocytic anemia
AUTOIMMUNE NEUROPATHY • Guillain-Barré syndrome (acute idiopathic polyneuritis) • Myasthenia gravis • Multiple sclerosis
Guillain-Barré syndrome • inflammation demyelinates peripheral nerves that causes progressive muscle weakness and paralysis • the cause is the loss of myelin • occurs often 1-3 weeks after infection (Campylobacter jej.) • features: progressive weakness and paresthesia of the lower and later upper extremitas and respiratory muscles, weakness can leads to paralysis and respiratory failure • immunologic findings: autoantibodies against gangliosidemembrane
Myasthenia gravis • chronic disease with impaired neuromuscular transmission • characterized by muscle weakness and fatigue • the muscle weakness and neuromuscular dysfunction result from blockageand depletion of acetylcholine receptors at the myoneural junction • immunological findings: autoantibodies against Ach receptors • ptosis of the eye