Download
1 / 51
510 likes | 525 Views
This presentation provides an outline of the role of faith-based health services in DR Congo, the challenges faced, and future perspectives. It also discusses the partnership between ECC-DOM and IMA World Health in providing essential health care services.

E N D
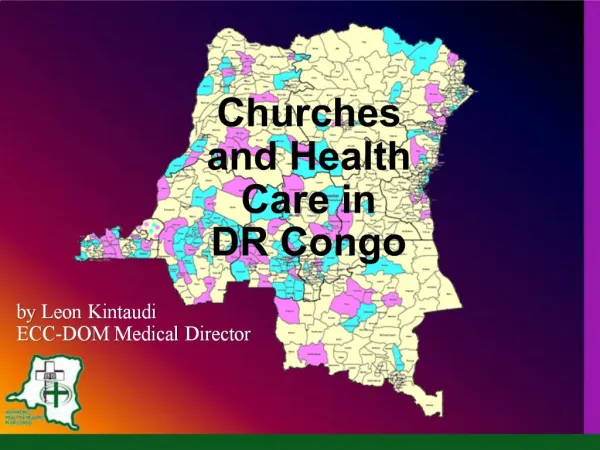
Churches and Health Care in DR Congo by Leon Kintaudi ECC-DOM Medical Director
Presentation Outline • ECC-DOM and IMA World Health • A Brief History of Health Zones • The Role of Faith-Based Health Services • Challenges and Future Perspectives
ECC-DOMProtestant Church of Congo Medical Office • 61 member communities • 80 hospitals • 600+ health centers • 70 co-managed health zones (see map)
IMAWH is a member association of twelve U.S. church relief and development agencies: – Adventist Development Relief Agency – Lutheran World Relief – American Baptist Church USA – Mennonite Central Committee – Christian Church (Disciples of Christ – Presbyterian Church (USA) – Church of the Brethren General Board – United Church of Christ – Church World Service & Witness – Episcopal Relief and Development – United Methodist Church, Global Min. – Vellore Christian Med College
The IMA World Health Mission To provide essential products and services for emergency, health and development programs of interest to member agencies which serve people in need without regard to ethnicity, creed, color, gender, national origin or religious or political affiliation.
ECC-DOM and IMA World Health • Operational Strengths • Collaboration with MOH • Procurement • Project management • Networking • Financial management
The Congo Health System… is well designed to provide comprehensive primary health care through decentralized health zones co-managed, in many cases, by churches & NGOs.
Health Zone Administrative Structure Central office : Health Zone Management Committee Hospital Director Supervision Health Center Management Committee Hospital Management Committee Health Post Health Center ReferralH.Center ReferralHospital Referral Referral Referral
Components of a Health Zone in DR Congo- 125,000 people- 20 Health Centers- 1 Ref. hospital
The Purpose of Health Zones is to provide Primary Health Care • Curative Care… treating the fever • Preventive Care… sleeping under a bednet • Promotional Care… draining swampy areas The challenge is to maintain a balance of resources
1975 National Workshop • Adopted concepts of decentralized Health Zones and primary health care. • Agreed on a principle of co-management by Government and church hospitals.
1984 – before HZ delimitation 75% of the first 85 health zones were developed around church hospitals
1984 – after HZ delimitation 75% of the first 85 health zones were developed around church hospitals
The Roles of FBOs in Health Care • Pioneering of community health services • Provision of PHC services at community level • Provision of Referral Services (hospitals) • Co-Management of Health Zones (~180) • Management of Regional Services (depots) • Management of National Projects (SANRU)
Co-Management Public vs. Private Co-management by FBOs & NGOs • ~50% of health services provided by FBOs / NGOs • ~50% of health facilities are owned by FBOs • HZs are MOH “owned” with FBO co-management
SANRU Rural HealthHZ Development Assistance • 1981-86 SANRU I 50 HZs • 1986-91 SANRU II 100 HZs • 1991-00 ECC/DOM 12-36 HZs • 2000-06 SANRU III & PMURR 75 HZs • 2006+ AXxes, PMURR, Global Fund 128 HZs
AXxes PMURR Abbott SP+ GF MRP DEVRU Health Development in 128 of DRC’s 515 health zones
SANRU the project has evolved into SANRU the Program ECC-DOM’s partnership with IMA World Health manages $10 million of assistance to health zones each year
ECC / IMAWH SANRU Program Objectives • Integrated Primary Health Care • especially for Mothers and Children • Health Systems Strengthening • of decentralized health zones, • especially those co-managed by FBOs • (including community & congregation
Actions through SANRU • Strengthening Integrated PHC • (pre-natal clinic, well child clinic, family planning, post-natal care, vaccination, etc) • Health education / C-IMCI • Water and Sanitation • Malaria prevention & treatment • Training health teams • Essential drugs supply • Health zone development
Malaria: Fever during last 14 days among households with and without ITNs n=514
Water, Sanitation & Hygiene2163 Springs capped – Access increased 32% Waterborne disease decreased by 30%
Challenges • Sustainability of HZs after projects end. • Stability of the country • Control of endemic diseases like Malaria, ARI, HIV/AIDS, Tuberculosis and Malnutrition • Knowledge and understanding of illness by the population
FUTURE PERSPECTIVES • Continue present activities in health zones • Continue collaboration with the MOH • Improve training (ST & LT) for health personnel • Improve income activities for HZs & population • Emphasize Maternal, Child & new born care • Identify funding for newly formed HZs and health zones without development partners.