Download
1 / 24
270 likes | 1.04k Views
Acute Pulmonary Edema During Emergence from Anesthesia. Liu, Chih-Min 2003-9-22. History. 51 y/o female 68 kg Past history: DM; HTN: noted > 2 years, under poor medical control Clinical diagnosis: Vitreous hemorrhage, L ’ t side Operation: PPV on 2003-9-17. ASA class lll E.

E N D
Acute Pulmonary Edema During Emergence from Anesthesia Liu, Chih-Min 2003-9-22
History • 51 y/o female • 68 kg • Past history: • DM; HTN: noted > 2 years, under poor medical control • Clinical diagnosis: Vitreous hemorrhage, L’t side • Operation: PPV on 2003-9-17
ASA class lllE • BP: 237/134 mmHg at the OR • Past history: • DM; HTN: noted > 2 years, under poor medical control
Induction • Fentanyl 100 micro-gram • Cis-atracurium 10 mg • Xylocaine 80 mg • Propofol 120 mg • Esmolol 25 mg
Maintain • Vital sign: • BP: about 110/60 mmHg • HR: 90/min • SpO2: • 92% at the beginning • 99% during operation • Medication: • Inhalation gas: Desflurane • Atropine: 0.5 mg • Nitroderm
Emergence • Medication • Atropine: 0.5 mg; Enlon:52 mg • Vital sign • BP: 250/135mmHg • HR: 90/min • SpO2: • Rapid drop to 60% • Respiration sound: • Bilateral rales • Heart sound: • Severe systolic murmur (4/6) at left 5th intercostal space
Emergence • Mask ventilation with pure O2 • Medication: • Trandate, Millisrol (bolus and infusion), Lasix, Morphine, Solu-cortef • Set A-line • Insertion of CVP (femoral vein) • Re-intubation • ICU
Induction • Emergence • SpO2: 60%
Medication • BP • Blood gas: • PO2: 83.9mmHg • PCO2: 58.6 mmHg • pH: 7.22 • SpO2: 93.6%
Chest X-ray • Bilateral pulmonary edema; Bilateral rales • Heart sound: • Systolic murmur
Send to ICU • Ventilator • SIMV • PEEP • Sedation
Lab data at ICU • CBC • WBC: 15340 • Cardiac enzyme • CK, CK-MB, Troponin I: within normal range • Blood gas: • (9/17) PO2: 192 mmHg • (9/18) PO2: 177 mmHg • Cardiac echo • LVEF: 70%, good
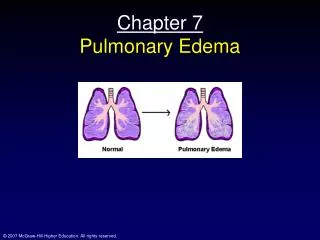
What happened? Pulmonary Edema
Etiology • Types • NEGATIVE-PRESSURE PULMONARY EDEMA (Permeability) • CARDIOGENIC PULMONARY EDEMA (Hemodynamic) • NEUROGENIC PULMONARY EDEMA • Which is most likely?
NEGATIVE-PRESSURE PULMONARY EDEMA • Also known as postobstructive pulmonary edema • Characterized by its rapid onset and short-lived course • Large, negative intrapleural pressures are the pathophysiologic hallmark of negative-pressure pulmonary edema • Various types of airway obstruction, including croup, epiglottitis, laryngospasm after tonsillectomy, hanging, and tumors have been reported • Symptoms commonly resolve within 12 to 24 hours • Suction mechanism
NEUROGENIC PULMONARY EDEMA • The exact cause of neurogenic pulmonary edema is unknown • Increased capillary hydrostatic pressure and increased capillary permeability • With a history of head trauma or intracranial pathology • CARDIOGENIC PULMONARY EDEMA • Develops when Pcap is excessively high, overwhelming the ability of the lymphatic system to resorb fluid. • Left-to-right shunting lesions, such as a patent ductus arteriosus or a ventricular septal defect • Ventricular function
Negative-pressure Pulmonary Edema in a Child with Hiccups during Induction[CASE REPORTS]Anesthesiology, 93(1): 282-4 • Negative-pressure pulmonary edema (NPPE) occurs soon after relief of acute or chronic obstruction of the upper airway. It is commonly reported after laryngospasm during induction or emergence from anesthesia. • Markedly negative intrapleural pressures during airway occlusion cause increased venous return and increased left ventricular afterload. The increased hydrostatic pressure gradient in the pulmonary capillaries leads to transsudation of fluid into the alveoli. Hypoxemia and a hypoxia-induced hyperadrenergic state further promote edema formation. • It is likely that more cases of unexplained perioperative hypoxemia are related to unrecognized NPPE.
Negative-pressure Pulmonary Edema in a Child with Hiccups during Induction[Correspondence]Anesthesiology, 94(2): 378-9 • NPPE v.s. CPE: • The most specific method for differentiating NCPE from CPE is the demonstration of increased alveolar–capillary permeability, which is characteristic of NCPE. Alternatively, pulmonary capillary wedge pressure measurement could be useful to differentiate CPE from NCPE. • Echo: • An echocardiogram shows normal left ventricular systolic and diastolic function in NCPE • X-ray • Centrally distributed pulmonary edema could be suggestive of cardiogenic origin
Pulmonary oedema associated with airway obstructionCanadian Journal of Anaesthesia. 37(2):210-8, 1990 Mar • Pathogenesis of pulmonary oedema associated with upper airway obstruction is multifactorial • negative intrapleural pressure is the dominant pathophysiological mechanism involved in the genesis of pulmonary oedema associated with upper airway obstruction • The majority of cases present within minutes • Resolution is typically rapid, over a period of a few hours. • Maintenance of a patent airway, supplemental oxygen, mechanical ventilation and positive end-expiratory pressure