Download

1 / 12
830 likes | 3.1k Views
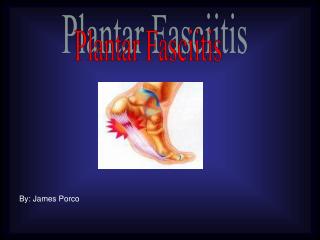
PLANTAR FASCIITIS. Patho-physiology. Repeated tensile and compressional stresses on the arched foot Fascial anatomy focusing stress into narrow band of fibrocartilage Cycles of tearing and healing Release of chemical mediators of inflammation, producing pain

E N D
Patho-physiology • Repeated tensile and compressional stresses on the arched foot • Fascial anatomy focusing stress into narrow band of fibrocartilage • Cycles of tearing and healing • Release of chemical mediators of inflammation, producing pain • Eventually, myxoid degeneration and weakening of the fascia • A pronated, flat foot and rarely a spontaneous rupture • Painful scar tissue and calcification (spur formation)
Risk Factors • Overweight • Middle-aged • Sedentary lifestyle • Reduced ankle dorsiflexion1 • Hard surfaces • Flat shoes • Human leucocyte antigen (HLA) B27 associated spondyloarthropathies
Pain BELOW the heel - ‘tearing’ above heel→ usually Achilles tendonitis dorsiflexion of toes and ankle causes radiates to forefoot/leg→ S1/S2 lesion pain - worst in morning - on weight-bearing Tenderness maximal at origin of fascia Dorsiflexion of toes and ankle causes pain Presentation
Treatment of Plantar Fasciitis The Slant-board Stretch & the Stair stretch
Treatment of Plantar Fasciitis Dynamic stretches such as rolling the foot arch over a can or a tennis balls are also useful. Cross-friction massage above the plantar fascia and towel stretchingmay be done before getting out of bed.
Splinting Some other treatments available are supports such as night splints which stretch the plantar fascia while you sleep. By stretching the plantar fascia, it will be forced to lengthen and avoid the early morning tightness and pain brought on by lack of use overnight while at rest.
Don’t Forget Unusual Things • Pain after 3-6 months not responding to treatment → Fibrosarcoma Foreign body Paget’s TB Gout