Download
1 / 60
620 likes | 655 Views
OSTEOARTHRITIS DIAGNOSIS AND MANAGENENT. Presented By: Fadel Naim M.D. Orthopedic Surgeon IUG. Osteoarthritis (OA):.

E N D
OSTEOARTHRITIS DIAGNOSIS AND MANAGENENT Presented By: FadelNaim M.D. Orthopedic Surgeon IUG
Osteoarthritis (OA): A chronic joint disorder in which there is progressive softening and disintegration of articular cartilageaccompanied by new growth of cartilage and bone at the joint margins (osteophytes) and capsular fibrosis.
Osteoarthritis(OA): • Differs from simple wear and tear • Asymmetrically distributed and often localized to only one part of a joint • Related to abnormal loading rather than frictional wear • Unaccompanied by any systemic illness • Not primarily an inflammatory disorder
Differentiating Features • Rheumatoid arthritis: • Young, small joints • Autoimmune • Synovial inflammation • Synovium cartilage • Osteoarthritis: • Old, large joints • Degenerative • Cartilage degeneration • Cartilage synovium
OA is a dynamic phenomenon; it shows features of both destruction and repair
Primary osteoarthritis • signaled by an imbalance between the synthesis and degradation of the matrix components • secondary osteoarthritis • mechanical destruction of cells and matrix due to blunt trauma may be the cause of
Mechanism Of Osteoarthritis • Disparity between stress applied to articular cartilage and strength of articular cartilage • Increased stress (F/A) • Increased load (BW or activity) • Decreased area (varus knee or dysplastic hip) • Weak cartilage • Age • Stiff • Soft (inflammation) • Abnormal bony support (AVN)
Prevalence • The commonest of all joint diseases. • a truly universal disorder, affecting both sexes and all races • Everyone who lives long enough will have it somewhere, in some degree
Causes • Aging: Most important "cause" of OA • Genetics: abnormal type II collagen gene • Weight - At the hip and knee, 4 time body weight is concentrated across weight bearing surfaces • Trauma • Metabolic Abnormalities: ( hemochromatosis, hypothyroidism, hyperparathyroidism, hypomagnesemia)
Components of a Comprehensive History • Symptom type • Pain • Swelling • Decreased range of motion • Mechanical • Crepitus • Locking • Pseudolocking • Catching • Giving way • Location of symptoms • Isolated Medial • Lateral • Patellofemoral • Diffuse • Symptom timing • Onset • Sudden • Insidious • Duration
Components of a Comprehensive History • Exacerbating or ameliorating factors • Symptom intervention and response • Lifestyle modification • Rehabilitation • Footwear • Assistive devices • Prior treatment • NSAIDs • Injections • Bracing • Rehabilitation • Surgery • Past medical history • Past surgical history • Family history
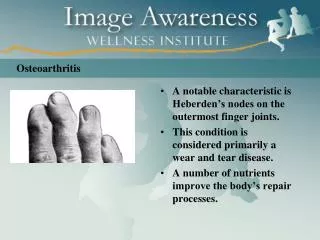
Clinical characteristics of osteoarthritis • Middle age. • Loss of function • Mild morning stiffness (<15 minutes) • Pain with use • Swelling • Gelling (stiffness after rest) • Boney deformity
ROM • Often painless within the permitted range • May be accompanied by crepitus
Stiffness is common; characteristically it occurs after periods of inactivity, but with time it becomes constant and progressive.
Swelling may be intermittent (suggesting an effusion) or continuos (with capsular thickening or large osteophytes)
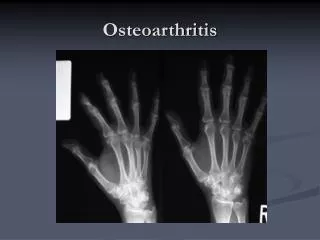
Radiographic features • Non-uniform joint space narrowing • Subchondral sclerosis • Subchondral cysts • Osteophytes A standing anteroposterior view with the patient's body weight evenly distributed on both legs is commonly obtained
The management is depending on? • the stage of the disorder • the severity of the symptoms • the age of the patient • his or her functional needs.
Goals Of Treatment • Decrease pain • Optimise mobility • Maximise quality of life • Reduce joint inflammation • Slow down disease progression • Maximise drug efficacy and minimise drug toxicity • Treat other organ damage outside the joints • Halt disease progression and regain lost function
EARLY TREATMENT The principles are: (1) Maintain movement and muscle strength (2) Protect the joint from ‘overload’ (3) Relieve pain (4) Modify daily activities
Nonsurgical treatment modalities include: • Lifestyle modification • Medical management • Bracing • Orthotics • Rehabilitation
Nonsurgical Modalities Lifestyle Modification Patient education is of primary importance for lifestyle modification to be effective.
Load reduction • weight reduction for obese patients • wearing shock absorbing shoes • Avoiding activities like climbing stairs • Using a walking stick • slow down the rate of cartilage loss • Effective in relieving pain
Limiting squatting and stair climbing reduces pain in patients with significant patellofemoral arthrosis
Adaptations in the home, such as raising the level of a chair or toilet seat, may become necessary for those with chronic symptomatic osteoarthritis of the knee
Footwear Energy-absorbing shoes or inserts may assist in reducing impact loads across the knee joint.
Sole modification or use of off-the-shelf wedge inserts can correct pronation or supination deformities during weight- bearing, leading indirectly to mechanical realignment Decreasing loads across the painful compartment may reduce symptoms.
Supportive Devices • The use of a cane in the hand contralateral to the affected limb to relieve force and reduce symptoms • A properly fitted cane should reach the top of the greater trochanter of a patient wearing shoes
Analgesic medication Pain relief is important • not all patients require drug therapy and those who do may not need it all the time. • Treatment should begin with the least expensive drug that has the least chance for side effects (such as paracetamol) • If this fails, a non-steroidal anti- inflammatory preparation may be better.
Pharmacologic Management • Acetaminophen • NSAIDs • Injectable corticosteroids • Injectable viscosupplementation • Chondroprotective oral supplements
Acetaminophen a first-line analgesic agent by the orthopaedic and rheumatologic communities • favorable side-effect profile • equivalent efficacy in relief of pain • 650 mg every 4 to 6 hours • maximum dosage of 4,000 mg per day. • A dose of 1,000 mg three or four times daily is usually sufficient
Nonsteroidal Anti-inflammatory Drugs The anti-inflammatory and analgesic actions of NSAIDs make them the preferred pharmacologic agent for the swollen and painful arthritic knee
Side effects of NSAID • Dyspepsia • gastrointestinal • ulceration • renal toxicity • hepatotoxicity • cardiac failure. dose-related and more severe in elderly individuals, with prolonged elimination
Chondroprotective Oral Supplements • Glucosamine stimulates chondrocyte and synoviocyte metabolism, • Chondroitin sulfate inhibits degradative enzymes and prevents formation of fibrin thrombi in periarticular tissues synergistic actions when taken together
Indications for Corticosteroid Intra-articular Injection • Failed first-line anti-inflammatory • therapy • Contraindications to use of acetaminophen or NSAIDs • Unresponsive to other nonsurgical modalities for a period of 6 to 8 weeks
Relief, lasting from a few days to 6 months or more, especially in the absence of mechanical symptoms Should be limited to a maximum of three or four per year After injection, patients should avoid strenuous or prolonged weight-bearing activities for 48 hours
Viscosupplementation • Usedsince 1987 in humans • Series of three and five weekly injections • Relief of pain may last from 0 to 24 months
Viscosupplementation • Synvisc, Hyalgan, Adant, etc. • Joint fluid in arthritis becomes abnormal • Loss of lubrication and viscosity
The mainstay of treatment in the early case is ? physiotherapy physiotherapy aims to: • maintaining joint mobility • improving muscle strength
Exercise that includes running and jumping should be avoided • Low-impact or non-impact activities, such as swimming, walking and bicycling, are excellent recommendations
Intolerable lifestyle changes or a poor response to non-operative management may ultimately dictate surgical treatment.