Download
1 / 18
430 likes | 1.92k Views
ATELECTASIS. By: Josephine Ekong #688. CONTENTS. Definition. PATHOPHYSIOLOGY. RISK FACTORS. TYPES. Clinical manifestation. PHYSICAL FINDINGS. TREATMENT. PROGNOSIS. DEFINITION. It is defined as partial or complete collapse of a lung.

E N D
ATELECTASIS By: Josephine Ekong #688
CONTENTS Definition PATHOPHYSIOLOGY RISK FACTORS TYPES Clinical manifestation PHYSICAL FINDINGS TREATMENT PROGNOSIS
DEFINITION • It is defined as partial or complete collapse of a lung. • It is also an incomplete expansion (neonatal atelectasis) or collapse of previously inflated lung providing relatively airless parenchyma.
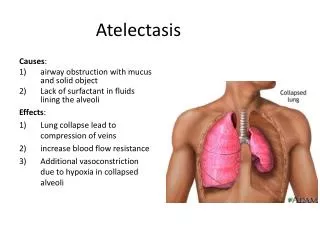
PATHOPHYSIOLOGY This occurs when there is a blockage of the air passages (bronchus) by mucus or masses or by pressure from outside of the lungs.
RISK FACTORS • Anesthesia • Foreign body in the airway • Lung disease • Mucus plugging of the airway • Pressure caused by mass or fluid • Prolonged bed rest • Shallow breathing (like when people splint secondary to rib fractures)
TYPES Resorption Contraction Compression
Resorption Atelectasis •Completeobstruction of an airway, whichleads to resorption of oxygen trapped inthe alveoli. • Caused by excessive secretions (mucousplugs) or exudates with in smaller bronchi. • Often found in bronchial asthma, chronicbronchitis, bronchiectasis, postoperative states, and aspiration of foreign bodies. •Mediastinum shifts towards atelectaticlung.
Contraction Atelectasis • Contraction atelectasis: local or generalized fibrotic changes in thelung or pleura prevent full expansion. Contraction atelectasis is irreversible. The other types of atelectasis are Reversible.
Compression Atelectasis • Compression atelectasis: pleural cavity ispartially or completely filled by fluid exudate, tumor, blood, or air. • Tension pneumothorax. •Cardiac failure Pts. develop pleural effusion. • Abnormal elevation of the diaphragminduces basal atelectasis • Mediastinum shifts away from the affectedlung.
CLINICAL FEATURES • Trouble breathing • Pleurisy (chest pain with inspiration) • Cough • Fever • Pneumonia CAN develop in an area of atelectasis.
PHYSICAL FINDINGS • Decreased breath sounds • Dull sound on percussion • Decreased fremitus • Tracheal deviation towards the side of lesion
TREATMENT • The goal is to expand the lung. • If fluid or an air leak (pneumothorax) is causing the trouble, then IT needs to be drained. • Other treatment includes: • Percussion of the chest:- clapping the chest can mobilize mucus plugging and allow for the airways to clear. • Incentive spirometry:- in this breathing exercise, the patient takes a deep breath deeply and slowly then hold the breath long enough to keep the disk raised for at least 3 seconds. Repeat at least once every hour.
Bronchoscopy:- by looking into the lungs and the pulmonary specialist can manually remove any movable blockage from the airway. • Postural drainage:- by changing positions, mucus and plugging can be relieved and thus improve the collapse of the airways. • PEP (positive expiratory pressure)device can open up clogged airways.
PROGNOSIS • In an adult, a small area of atelectasis is not life threatening or even serious. The rest of the lung can make up for this area in terms of oxygenation and CO2 exchange. • Large areas of atelectasis can be serious. Specially if the patient has other illness or lung problems. Small children are particularly at risk of complications.
REFERENCES • Dr. RotimiM.D, Windsor Unisch of Medicine, faculty of Medical Pathology, Jan – April 2014 • RosenbloomSA, Ravin CE, Putman CE, et al. Peripheral middle lobe syndrome. Radiology. 1983;149:17-21. [Medline]. • Priftis KN, Mermiri D, Papadopoulou A, Anthracopoulos MB, Vaos G, Nicolaidou P. The role of timely intervention in middle lobe syndrome in children. Chest. Oct 2005;128(4):2504-10. [Medline]. • O’Donnell AE. Bronchiectasis, atelectasis, cysts, and localized lung disorders. In: Goldman L, Schafer AI, eds. Cecil Medicine. 24th ed. Philadelphia, Pa: Saunders Elsevier; 2011:chap 90.