Download
1 / 30
320 likes | 559 Views
Medical Treatment for Osteoporosis ~ From today to tomorrow. Presented by 劉明æ‘. Miacalcic. Qualitative Effects of Salmon Calcitonin Therapy (QUEST). NIH Definition of Osteoporosis.

E N D
Medical Treatment for Osteoporosis ~From today to tomorrow Presented by 劉明村
Miacalcic Qualitative Effects of SalmonCalcitonin Therapy (QUEST)
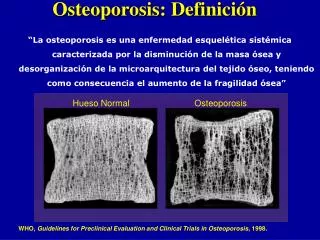
NIH Definition of Osteoporosis Osteoporosis is defined as a skeletal disorder characterized by compromised bone strength predisposing a person to an increased risk of fracture. Bone strength primarily reflects the integration of bone density and bone quality. Normal bone Osteoporosis NIH Consensus Development Panel on Osteoporosis. JAMA 285 (2001): 785-95
Bone quantity vs bone quality: Evolution of the paradox Decrease in vertebralfracture risk (%) Increase invertebral BMD (%) Treatment Fluoride1 Raloxifene2 Salmon calcitonin3 Risedronate4 Alendronate5 Strontium-ranelate6 0 30 36 41 47 41 35 2–3 1–1.5 3–5 6–8 14 BMD: Bone mineral density 1. Riggs BL et al.N Engl J Med. 1990;322:802–9 2. Ettinger B et al.JAMA. 1999;282:637–45 3. Chesnut C III et al.Am J Med. 2000;109:267–76 4. Harris ST et al.JAMA. 1999;282:1344–52 5. Black DM et al. Lancet. 1996;348:1535–41 6. Meunier P et al. N Engl J Med. 2004;350;459-68
The importance of architectural integrity Normalbone 10% decrease in BMD due to loss in trabecular thickness equals 20% reduction in bone strength 10% decrease in BMD due to loss in trabecular number equals 70% reduction in bone strength Silva MJ. Gibson LJ. Bone. 1997:21;191–9 Parfitt AM. Am J Med. 1991; 91 (Suppl5B):42S-46S.
Conclusion Thus, based on BMD alone, anti-resorptive agents that induce a greater increase in BMD cannot be assumed to be more efficacious in reducing fracture risk than those producing a lower BMD increase. Riggs BL, Melton LJ III. J Bone Miner Res 2002;17:11–4
Study design • 2-year, double-blind, randomized, placebo-controlled study • Miacalcic 200 IU NS vs placebo NS • All patients received calcium 500 mg daily • 91 postmenopausal women • At least 5 years post menopause • 1–5 vertebral fractures at baseline
Bone turnover – serum CTx Difference to placebo in serum CTx in the QUEST Study(*p < 0.05) QUEST study1 2 years 0 -5 -10 -15 Change vs placebo (%) -20 * -25 -30 serum CTx -35 -40 1. Chesnut CH III et al. J Bone Miner Res. 2005; in press 2. Srivastava A et al. Calcif Tissue Int. 2004;75:477-81
BMD data from QUEST and PROOF Difference to placebo in BMD at the lumbar spine in the QUEST and PROOF studies at 2 years 1.6 1.4 1.2 1.0 Median change vs placebo (%) 0.8 0.6 0.4 0.2 0.0 QUEST study / 2 years PROOF study / 2 years 1. Chesnut CH III et al. J Bone Miner Res. 2005 in press 2. The Proof study. Data on file
3D visualization from high-resolution MRI 36-year-old male (BV/TV = 0.28) 69-year-old male (BV/TV = 0.14) BeufO, Ghosh S, Newitt DC et al. Arthritis Rheum 2002;46:385–93
Bone microarchitecture MRI of the radius Only trabecular structures were evaluated • Region 1 is 7 mm from the distal endplate • Regions 1–4 are each 2.5 mm thick (corresponding to 5 MRI slices) Region 1 Region 2 Region 3 Region 4
Radius MRI: Trabecular bone volume 6 4 2 0 -2 -4 -6 -8 -10 -12 -14 Mean percentage change in apparent trabecular bone volume (BV/TV) from baseline to 24 months p = 0.01 p = 0.03 * Mean % change Miacalcic Placebo *** *** Region 1 Region 2 Region 3 Region 4 Change from baseline within group: *p < 0.05; ***p < 0.005
Radius MRI: Trabecular number Mean percentage change in apparent trabecular number from baseline to 24 months p = 0.01 p = 0.05 p = 0.01 ** Mean % change Miacalcic Placebo *** *** Region 1 Region 2 Region 3 Region 4 Change from baseline within group: **p < 0.01; ***p < 0.005
Radius MRI: Trabecular spacing 16 14 12 10 8 6 4 2 0 -2 -4 -6 Region 1 Region 2 Region 3 Region 4 Mean percentage change in apparent trabecular spacing from baseline to 24 months p = 0.01 Miacalcic Placebo p = 0.01 Mean % change ** ** * Change from baseline within group: *p < 0.05; **p < 0.01
Bone quality: Microarchitecture MRI of the hip (trabecular bone) Four regions of the hip were analysed: • Femoral Neck • Ward’s triangle • Upper trochanter • Lower trochanter
Femoral neck Ward’s triangle Upper trochanter Lower trochanter Hip MRI Mean percentage change in T2*, from baseline to 24 months *** Miacalcic p = 0.049 Placebo * *** Mean change from baseline (%) *** Change from baseline within group: *p < 0.05; ***p < 0.005
Conclusions Treatment with Miacalcic 200 IU NS for 2 years demonstrated • Improvements (vs. placebo) in bone quality (i.e. BV/TV, trabecular number and spacing) in the forearm (radius), as measured by MRI • Improvements in bone quality (vs. placebo), expressed by T2 ( decreased 2.6–7.4% relative toplacebo)at the hip (femoral neck, Ward’s triangle, upper and lower trochanters), statistically significant at the lower trochanter • BMD increase of 0.8% (ns) at the lumbar spine vs. placebo • 26% decrease in bone resorption (p < 0.05), as evaluated by serum CTx • No differences in the bone formation marker (serum BSAP) compared to placebo
Miacalcic 產品特色 對於治療骨折急性期伴隨骨痛的骨質疏鬆症患者 Miacalcic(密鈣息) 是: • 第一線的快速有效止痛且安全的鼻噴劑藥物, 它提供增加β-endorphine濃度,達到止痛的效果,減少臥床情況。 • Miacalcic長期使用可減少骨質流失; 增加骨密度與骨品質(PROOF and QUEST); 預防再次骨折,增加生活品質。
處方 Miacalcic 之建議 健保局給付規範 5.5.2. 抑鈣激素製劑 (Salmon calcitonin nasal spray, injection) 限惡性疾病之高血鈣症或變形性骨炎 (Paget‘s disease) 或停經後骨質疏鬆症引起之骨折 請先了解在處方 Miacalcic 前,是否已完成下列事項: 1. 是否病人已完成骨鬆檢查 (DXA<-2.5) (需提及為骨質疏鬆症) 2. 是否詳述病人年齡及性別 (需說明停經多久) 3. 是否有骨折(需附骨折部位之X光片) 4. 不得併用 Fosamax , Actonel , Evista , Vitamine D3 5. 是否詳述症狀 - 疼痛嚴重性 , 疼痛多久及部位 , 活動能力 6. 請說明病人已經用過同藥理之常用藥品無效,並舉出藥品名稱
Zoledronic Acid:Annual Bone Health management for Osteoporosis ~ From Cancer treatment to Paget’s Disease and PMO treatment ~
Molecular Structure of Zoledronic Acid • Zoledronic acidis a potent nitrogen–containing bisphosphonate • Core bisphosphonate moiety (red arrows) • R2 side chain: imidazole ring (blue arrows) OH O N P N OH C O OH P OH HO Green JR, et al. J Bone Miner Res. 1994;9:745-751.
Proposed Mechanism of Local Recycling of Zoledronic Acid in Bone O OH = P OH N N OH HO P BP BP OH = O ZOL has long duration of action Low desorption Avid uptake High re-attachment through recycling BP BP BP Zoledronic acid has high affinity for bone mineral leading to: High-affinity BPs may diffuse less well in bone and remain nearer accessible surfaces G Russell (2005).
Zoledronic Acid: Key Pharmacological Characteristics 0.5 0.4 0.3 0.2 0.1 0.0 • High binding affinity for bone in vitro • Maximizes attachment • Minimizes detachment • Potent FPP synthase inhibition in vitro • Maximizes antiresorptive potential • Minimizes total amount of drug required • Allows single administration of total annual dose Binding to Hydroxyapatite1 4 3 KL (L/mol x 106) 2 1 0 CLO ETD RIS IBA ALN ZOL rhFPP synthase2 IC50 (mM) ALN IBA RIS ZOL • Nancollas GH, et al. Bone. 2006, in press. • Dunford JE, et al. J Pharmacol Exp Ther. 2001;296:235-242.
Pharmacological Properties of Zoledronic Acid • Achieves prolonged suppression of bone resorption • No deleterious effect on bone quality • Increases bone mineral density • Reduces bone turnover • Does not impair mineralization • Has favourable effects on structural & mechanical properties of bone • IV administration does not blunt bone anabolic response to PTH
Zoledronic Acid Demonstrated Broad Efficacy in Women With Postmenopausal Osteoporosis • In women with postmenopausal osteoporosis, once yearly infusion of ZOL 5 mg over 3 years significantly reduces1: • Vertebral fractures (morphometric 70%, clinical 77%)1 • Hip fractures (41%)1 • Non-vertebral fractures (25%)1 • Days of disability due to fracture or back pain2 • Height loss1 • Significantly superior to placebo in increasing or preserving BMD1 • Markers of bone formation and resorption were reduced and maintained within premenopausal reference range over 36 months1 • Generally well tolerated1 • Fracture efficacy coupled with high adherence suggests potential role for ZOL 5 mg as treatment for osteoporosis1 1. Black DM, et al. N Engl J Med. 2007;356:1809-1822. 2. Black DM, et al. Presented at: ASBMR 28th Annual Meeting; September 15-19, 2006; Philadelphia, Pa. Abstract 1054. (n=7,736)
The HORIZON Recurrent Fracture Trial *Lyles KW, et al. N Engl J Med. 2007;10.1066:1-11.
Recurrent Fracture Trial Study Conclusions • Zoledronic acid*: • significantly reducedrisk of overall clinical fracture by 35% and multiple clinical fractures by 33% • significantly reduced mortality risk by 28% • significantly reducedrisk of clinical vertebral and non-vertebral fractures by 46% and 27%, respectively • had a 30% lower risk in hip fractures compared to placebo (NS) • significantly increased/preserved total hip and femoral neck BMD at all time points • showed comparable incidence of AEs and SAEs to placebo • demonstrated no evidence of long-term effect on renal function • demonstrated a 20% reduction in risk of atrial fibrillation/atrial flutter SAEs (n=12, 1.1%) relative to the placebo (n=15, 1.4%) • No adverse effects on fx. healing or ONJ risk (n=2,127; men and women) *Lyles KW, et al. N Engl J Med. 2007;10.1066:1-11.
Zoledronic Acid will Improve Patient Compliance as Once-Yearly IV Therapy is Preferred 66.4 More convenient 18.0 15.6 Once-Yearly IV Both Are Equal 59.8 More satisfying Once-Weekly Pill 20.5 18.9 68.0 More willing to take long term 16.4 15.6 66.4 Overall preference 13.9 19.7 0 20 40 60 80 100 % of Patients N = 122 Data from Lindsay R, et al. Poster presented at ECCEO6; March 15-18, 2006; Vienna, Austria.
Thanks for your attention! Aclasta is coming soon……