Download
1 / 11
110 likes | 234 Views
Influence of Timing of Clopidogrel Treatment on the Efficacy and Safety of Bivalirudin in Patients With NSTE-ACS Undergoing PCI. An Analysis of the ACUITY Trial Lincoff AM, JACC Intv 2008;1:639–48. PCI Subgroup. Background.

E N D
Influence of Timing of Clopidogrel Treatment on theEfficacy and Safety of Bivalirudin in Patients WithNSTE-ACS Undergoing PCI An Analysis of the ACUITY Trial Lincoff AM, JACC Intv 2008;1:639–48
PCI Subgroup Background • In REPLACE-2 (elective or urgent PCI), bivalirudin was not inferior to heparin plus a GP IIb/IIIa inhibitor in reducing ischemic events and the efficacy of bivalirudin was not influenced by the timing of clopidogrel administration1 • In contrast, preliminary analysis of the ACUITY trial found an interaction of borderline significance (p= 0.054) between clopidogrel exposure and randomized therapy on 30-day composite ischemia,2 leading to the suggestion that the use of bivalirudin monotherapy should be limited to NSTE ACS patients in whom clopidogrel pre-treatment is given . • This post-hoc analysis of the ACUITY trial, evaluated the timing of the initiation of clopidogrel treatment in patients undergoing PCI to determine whether clopidogrel pre-treatment is especially beneficial or necessary in patients not receiving a GP IIb/IIIa antagonist. 1: Saw et al 2. Stone GW. NEJM Lincoff AM, JACC Intv 2008;1:639–48
PCI Subgroup Method of analysis for clopidogrel timing study • Timing for the initiation of clopidogrel was a priori designated as: • Pre-angiography if initiated at any time prior to the angiography • Peri-PCI if initiated after angiography and within 30 minutes of the end of PCI • Post-PCI if initiated > 30 minutes after PCI • No clopidogrel. Patients who did not receive clopidogrel (or ticlopidine) at any time before or after PCI. Lincoff AM, JACC Intv 2008;1:639–48
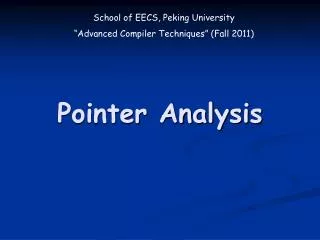
PCI Subgroup Clopidogrel at hospital pre- randomization N= 2383 Clopidogrel pre-hospital N=1820 Clopidogrelstudy population All ACUITY patients N= 13,518 Medical management N= 4491 CABG N= 1539 PCI patients N= 7789 Missing data N=47 No clopidogrel N= 129 Underwent PCI and received clopidogrel at some time prior to or during hospitalization N= 7517 Ticlopidine N=96 Pre-angiography cohort Peri-PCI cohort Post-PCI cohort No clopidogrel Known dose and duration Clopidogrel post-PCI N=814 Clopidogrel pre-angiography N= 928 Clopidogrel peri-PCI N=1572 Lincoff AM, JACC Intv 2008;1:639–48
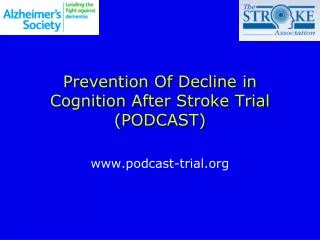
PCI Subgroup 30-Day Ischemic Outcomes • Analysis by clopidogrel timing and randomized treatment arm P=0.08 GPIIb/IIIa plus heparin 23.3 GPIIb/IIIa plus bivalirudin 20 19.5 Bivalirudin alone P=0.13 P=0.29 P=0.46 % Composite Ischemia 12.6 8.9 10.8 9.5 10 8.8 8.9 8.6 8.5 8.1 6.9 0 Pre-procedure N=5131 Peri-PCI N=1572 Post-PCI N=814 None N=129 Timing of Clopidogrel Exposure Lincoff AM, JACC Intv 2008;1:639–48
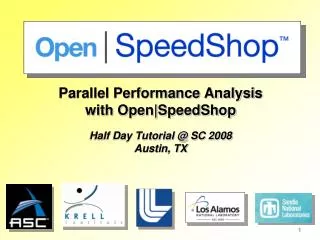
PCI Subgroup 30-Day Ischemic Outcomes • Analysis by clopidogrel timing and randomization to bivalirudin alone vs combined heparin or bivalirudin plus GPIIb/IIIa P=0.18 23.3 GPIIb/IIIa antagonist + any anticoagulant 20 Bivalirudin alone P=0.22 14.0 12.6 P=0.77 Composite Ischemia % P=0.36 9.7 8.8 8.6 10 8.1 8.2 8.8 0 Pre-PCI N=5131 Peri-PCI N=1572 Post-PCI N=814 None N=129 Timing of Clopidogrel Exposure Lincoff AM, JACC Intv 2008;1:639–48
PCI Subgroup 30-Day Ischemic Outcomes in Troponin+ PCI Patients • Analysis by clopidogrel timing and randomization to bivalirudin alone vs combined heparin or bivalirudin plus GPIIb/IIIa P=0.72 23.1 GPIIb/IIIa antagonist + any anticoagulant 20 19.6 P=0.13 Bivalirudin alone 13.7 Composite Ischemia % P=0.60 P=0.97 9.0 9.1 10 8.4 8.3 8.2 0 Pre-PCI N=2824 Peri-PCI N=950 Post-PCI N=471 None N=77 Timing of Clopidogrel Exposure Lincoff AM, JACC Intv 2008;1:639–48
PCI Subgroup Estimated Spline Transformation and 95% C.I. 2 1 GPIIb/IIIa antagonist + any anticoagulant Log Odds for Composite Ischemia (30-Days) 0 Bivalirudin alone -1 -2 -3 -4 0 2 4 6 8 10 12 14 16 18 20 22 24 Duration of Clopidogrel Treatment Prior to PCI (hours) 30-Day Ischemic Outcomes • Patients with known time of clopidogrel administration (n=928) • Analysis by duration of cloplidogrel treatment pre-PCI and randomization to bivalirudin alone vs combined heparin or bivalirudin plus GPIIb/IIIa Lincoff AM, JACC Intv 2008;1:639–48
Outcomes and clopidogrel administration Pre* - or Peri† -PCI PCI Subgroup Bivalirudin monotherapy better (N=2284) UFH/enoxaparin + GP IIb/IIIa better (N=2189) Groups based on first exposure to clopidogrel; excludes patients who received ticlopidine. *Pre-PCI = patients who received clopidogrel either prehospital, prerandomization, postrandomization, or preangiography. †Periprocedural = patients who received clopidogrel after angiography and within 30 minutes after PCI procedure. Lincoff AM, JACC Intv 2008;1:639–48
Outcomes and clopidogrel administration Post-PCI‡ or None§ PCI Subgroup Bivalirudin monotherapy better (N=290) UFH/enoxaparin + GP IIb/IIIa better (N=317) Groups based on first exposure to clopidogrel; excludes patients who received ticlopidine. ‡Postprocedure = patients who received clopidogrel any time >30 minutes after PCI within the index hospitalization. §No clopidogrel = patients who had no documentation of receiving clopidogrel at any time before or after the PCI procedure. Lincoff AM, JACC Intv 2008;1:639–48
PCI Subgroup Conclusions • In ACUITY, patients who received clopidogrel either prior to, or at the time of PCI achieved similar ischemic event rates and significantly less bleeding when randomized to bivalirudin alone vs a GPIIb/IIIa antagonist, irrespective of troponin status. • Among patients for whom clopidogrel will be given more than 30 min or not at all after PCI, an antithrombotic regimen that includes GP IIb/IIIa inhibition may provide better protection against ischemic events than does bivalirudin alone. • These data are reassuring for the treatment of patients with NSTE-ACS who undergo diagnostic catheterization and PCI with bivalirudin alone without clopidogrel pre-loading Lincoff AM, JACC Intv 2008;1:639–48