Download
1 / 50
500 likes | 605 Views
SCI Overview: Demographics, Terminology, Clinical issues, & Research Approaches. William McKinley MD Dept. of PM&R Director SCI Rehabilitation Medicine. Epidemiology of SCI. Incidence: 40 cases per million Prevalence: 200,000 currently in USA 200 new SCI / year in Virginia 80/yr at VCU

E N D
SCI Overview: Demographics, Terminology, Clinical issues, & Research Approaches • William McKinley MD • Dept. of PM&R • Director SCI Rehabilitation Medicine
Epidemiology of SCI Incidence: 40 cases per million Prevalence: 200,000 currently in USA 200 new SCI / year in Virginia 80/yr at VCU 61% Traumatic (MVA, Violence, Fall) 39% Nontraumatic (SS, Neoplasm, ischemia)
Epidemiology (Cont.) • Demographics: Age: 31 yrs, 82% male, 56% Caucasian, 63% employed, 54% single (NT/SCI older, male = Female) • Etiology: MVA 37%, Violence 28%, Falls 21% • 90% discharged to home • Costs: $40-100K (Acute) - $500K (lifetime) • Life Expectancy: lower than average • Cause of Death: Pulmonary, Cardiac
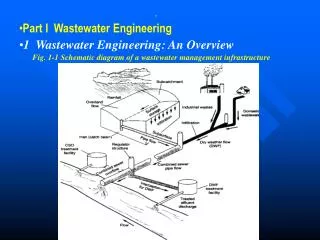
Model Spinal Cord Injury Care System Locations *Currently funded systems
SCI Model Systems • 5 yr ( $1.8 million) • Objectives • clinical continuum of care • national data collection • focused research (VCU: Employment) • collaborative research
VCU SCI Research • Etiology & Rehab Outcome Studies • violent/nonviolent • nontraumatic/traumatic • Secondary Issues • medical complidations • depression/grief • substance abuse • Community Reintegration • employment / recreation
Key Terminology • Tetraplegia/Paraplegia • Neurologic Level of Injury (NLOI) • most caudal normal M/S level (ie: C-5) • Zone of Injury • 3 levels distal to NLOI • Complete vs Incomplete • ASIA Classification
ASIA Impairment Scale • A = Complete – No Sacral Motor / Sensory • B = Incomplete – Sacral sensory sparing • C = Incomplete – Motor Sparing (<3) • D = Incomplete – Motor Sparing (>3) • E = Normal Motor & Sensory
Neurological Recovery Following SCI • Zone of Injury (ZOI) • Peripheral Nerve root (PNS) regeneration (1 year) • “Below ZOI” (Incomplete SCI) • Neuropraxic recovery (1-3 months) • Peripheral Sprouting (3-6 months) • Muscle Hypertrophy (3-6 months)
Neurological Recovery w/in the Zone of Injury • Prognostic indicators: • Incomplete > Complete(motor > pin > light touch) • Time post-injury • Rate of change
Prognosis for “Functional” (ASIA D) Recovery (below ZOI) • Complete (ASIA A) 0-5% • Sensory Incomplete (ASIA B) 20% • Sensory Incomplete (ASIA B-2) 40% • Motor Incomplete (ASIA C) 60%
Other Prognostic Factors • Mechanism of Injury: • Unil fact dislo > Flexion-Rotation • Etiology: • Spinal stenosis > GSW • MRI: local edema > hemorrhage, transection • SSEP – no better than clinical exam
Clinical Impairments After SCI • Motor • Sensory • Bladder/Bowel • Sexuality • Autonomic Nervous System
Medical Complications of SCI • Infections (lung, GU) • Spasticity • Pressure Sores • Pain • DVT / PE • Orthostasis • Autonomic Dysreflexia
Functional Impairments • Mobility • walking, wheelchair, transfers • Activities of Daily Living (ADL’S) • dressing, feeding, grooming • Functional Independence Measure (FIM) • 1-7 rating scale for function (Dep….Indep)
Functional Abilities • C1-C5 motorized W/C • C-5 feeding • C6 manual W/C • C7 key level for functional Independence (transfers, dressing) • C8-T1 finger function • L2/3 ambulation
Post-Traumatic Changes to the Spinal Cord • “Primary” injury – Immediate nerve damage will lead to nerve degeneration • “Secondary” injury – Delayed nerve injury due to inflammatory response, ischemia, ca++, free radicals • Complete is NOT “complete” • Transection is rare • 10% can support substantial function
Post-Traumatic SCI changes • Primary cell loss • Secondary Cell loss • central hemorrhage/ischemia • wallarian degeneration • Cystic degeneration • Syringomyelia • Muscle atrophy • especially w/LMN loss
Prognosis following SCI • Nerve regeneration - “currently” this does not occur within the CNS • Neurological recovery - can occur in incomplete injuries and w/I the ZOI • Functional improvements - occur in relation to LOI, comp/inc, motivation, staff training, decreased complications
Why No SCI Regeneration? • 1. No stimulus for regeneration • Nerve Growth Factors (NGF) • (Levi-Montalcini, Nobel Prize) • PNS has NGF, CNS does not • Produced naturally • Protects against cell damage • Stimulates regeneration
Why No SCI regeneration (cont) • 2. Inhibitory Factors • Oligodendrocytes inhibit axon growth (Schwab-1980’s) • Antibodies can block this inhibition • 3. Impenetrable Regions • Astrocyte scars can block regeneration
SCI Research Approaches • 1. prevent secondary CNS cell death • 2. Promote Regeneration & Remyelination • 3. Prevent inhibition • 4. Maximize Function (despite impairment)
1. Clinical / Pharmacological Studies to prevent secondary Injury • randomized, multi-center trials • outcome measurements: • neurological improvement • ASIA, MIS • functional improvement (FIM) • walking, bladder, bowel, sexuality • decreased medical complications • spasticity, pain
Methylprednisilone (MP): steroids • Dual mechanism of action: • antioxidant: inhibits lipid peroxidation • anti-inflammatory: reduces vascular permeability • NASCIS - National Acute Spinal Cord Injury Studies
NASCIS 1 (early 1980's) • 330 patients (double blind randomized, multi-center) • compared high (1,000mg/day) and low (100mg/day) dose MP within 48-72 hours x 10 days • results: *No significant difference between high and low MP and more wound infections in the high dose group
NASCIS 2 (“Bracken protocol”- late 1980's) • 470 patients compared both within 8 hours and between 8-12 hours • compared high dose MP (30mg/kg bolus and 5.4mg/kg/h x 23 hrs) vs Naloxone and placebo • Results: * MP within 8 hours had significantly greater motor and sensory recovery than placebo, Naloxone and 8-12 hour group
NASCIS 3 (mid-1990's) • comparison of MP with Tirilazed • Tirilazed inhibits lipid peroxidation without glucocorticoid fx • Results: *MP for 48 hours has beneficial effects.Tirilazed at 48 hours similar to MP at 24 hours. Apparent role of lipid peroxidation
Gangliosides (Geisler 1991) • GM 1- neuroprotective properties, acts on intracellular calcium • 34 pts with 100mg iv daily x 26 days • Results: *GM 1 patients showed improved LE ASIA motor scores at 1 yr
Sygen (Ganglioside) study (mid-1990's) • 720 patients, acute and 12 mo f/u • 100 or 200mg daily for 58 days • Results: neurological improvement @ 1 year no different than placebo
4-Aminopyridine (4AP) • selectively blocks K+ channels in cell membranes • improves conduction by prolonging AP • allows propagation through damaged zones • normal half-life 3-4 hours
4AP Clinical studies • Multiple Sclerosis Studies • Fampridine (Phase II) SCI study • randomized, blinded study • potential benefits: improve spasticity, bladder, pain, motor • ? Adverse events: agitation, insomnia, seizures
Other Non-pharmacologic trials (to prevent 2nd injury) • Surgical decompression • acute decompression of sp cord • lack of randomized prospective trials • ? Incomplete > Complete SCI • ? timing (4-6 hours), risk factors • Hypothermia • decreases metabolic requirements • delayed development of hypoxia • decreased glutamate & free radical release • animal studies seem encouraging
SUMMARY: Prevention of Secondary Injury • MP (Bracken Protocol) • ? Gangliosides, 4-AP • ? surgical decompression, new drugs, hypothermia
2. Nerve Regeneration Research • stimulate outgrowth in appropriate directions • overcome anti-regenerative characteristics of adult CNS • inhibition (Anti-Nogo) • scar/ impenetrability (Chondroitinase) • convert nerve growth into functional reinnervation
Aguayo et. al. (1980's) • Transplanted CNS into PNS – Regeneration occurs! • * Axons need “permissive” environment • * Schwann cells are critical (NGF’s) • * results: electrically active small-diameter unmyelinated axon regeneration
Current Spinal nerve graft strategies • Transplantation • peripheral nerve tissue • fetal cells • Genetic precursor cells • NGF’s, myelin, Antibodies
Remyelination Research • Schwann Cell & PNS transplants • Transplanted embryonic stem cells • produce oligodendrocytes • M-1 antibodies stimulate remyelination
3. Removal of inhibition (Schwab) • Oligodendrocyte inhibitory proteins • inhibit axon growth and myelin formation • when treated with antibodies - increased axon regeneration in rats
SUMMARY: Nerve Regeneration • CNS axons need • permissive environment (NGF’s) • Removal of inhibitions • Nerve grafts allow for limited regrowth • ? functional connections
4. Maximize Function (Clinical Research studies) • Prevention & management of acute & chronic medical complications • Rehabilitation Outcome studies • Community reintegration & employment
Clinical Research • Bladder, spasticity, neuropathic pain • FES • Reversing learned non-use • biofeedback • body-weight supported ambulation (BSA)
Technological advances & enhancing function • Functional Electrical Stimulation (FES) - • Diaphragm - phrenic n stim (resp) • Lower ext.- “Parastep” (walking) • Upper ext. - “Freehand” (grasp) • Bladder - FES (voiding) • Implantable pumps (spasms, pain)
Current Clinical Trials • Fetal SC transplants to treat progressive syringomyelia • 4-AP for chronic SCI • Neurotropin-secreting transplants • Neural stem cell Tx in chronic SCI • Alternating electrical current sti • Supported treadmill ambulation • Nerve bridging
SUMMARY: Future Scenario (Combination Therapies) • Prevent secondary injury • steroids • Enhance Regeneration & Remyelination • nerve grafting, NGF’s, overcoming inhibition, guiding axons to target • Enhance Restoration • (Rehabilitation, 4 AP, FES, BSA) • ? Future opportunities • Vaccines (neuroprotection), stem cells
Preparing for research • Avoid irreversible surgical procedures • Prevent complications • atrophy (muscle, bone, neuronal) • contractures • Revearse learned non-use & atrophy • PT, FES, BSA, biofeedback