Download
1 / 46
460 likes | 553 Views
Cost Effectiveness of Outreach Interventions for Low-Income Multiethnic Women. Todd Wagner, VA & Stanford Rena Pasick, UCSF Stephen McPhee, UCSF Jeanne Mandelblatt, Georgetown Clyde Schechter, Albert Einstein SOM. Funded by NCI. July 27, 2005. Trends in Breast and Cervical Cancer.

E N D
Cost Effectiveness of Outreach Interventions for Low-Income Multiethnic Women Todd Wagner, VA & Stanford Rena Pasick, UCSF Stephen McPhee, UCSF Jeanne Mandelblatt, Georgetown Clyde Schechter,Albert Einstein SOM Funded by NCI July 27, 2005
Trends in Breast and Cervical Cancer • Breast cancer between 1990 and 2000 • age-adjusted mortality declined 2.3% per year • incidence increased ~0.4% per annum • Cervical cancer 1992-1999 • age-adjusted annual incidence declined by 9.3% • mortality rates declined by 2.3% SEER data: Ries L, Eisner M, Kosary C, et al. Cancer Statistics Review, 1975-2000. Bethesda, MD: National Cancer Institute; 2003.
What is Driving these Changes? • May be caused by diagnostic technologies • Mammogram • Papanicolaou (Pap) smear • Collinear with changes in • Record keeping • Natural changes in disease / other risk factors
Belief in Diagnostics • USPSTF and many health plans endorse the use of mammography and Pap smear • Debates about benefits of mammography See: Gotzsche and Olsen Lancet. Jan 8 2000;355(9198):129-134. Lancet. Oct 20 2001;358(9290):1340-1342. Lancet. Jul 27 2002;360(9329):338-339
Breast Cancer Incidence Ries L, Eisner M, Kosary C, et al. Cancer Statistics Review, 1975-2000. Bethesda, MD: National Cancer Institute; 2003.
Cancer Screening Promotion • Health providers frequently use: • Outreach (e.g., patient reminders): encourages women to see their provider for a mammogram (or Pap) • Inreach (e.g., physician reminders): reminds the physician to schedule a mammogram (or Pap)
Role of race/ethnicity • There are notable disparities by race/ethnicity • Disentangling the influence of biologic and socio-economic factors is the subject of considerable debate • Physician reminders assumes access, but disparities in access exist • Unknown whether patient reminders are equally effective across racial/ethnic subgroups
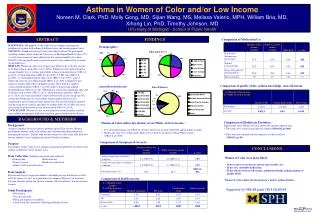
Project 1 • Project 1: we assessed the cost effectiveness of providing individually and culturally tailored printed health guides and telephone counseling to improve periodic breast and cervical cancer screening among low-income multi-ethnic women
Methods • Randomized, controlled cohort study • Modified random digit dialing (Mitofsky-Waksberg) • Targeted 86 low-income and ethnically diverse census tracts in Alameda county
Eligibility • Age 40-74 • African American, Chinese, Filipina, Latina, or non-Hispanic white • Speak English, Cantonese, Tagalog, or Spanish • Residence in a targeted census tracts • No history of cancer • Willingness to be randomly assigned to an intervention or control group, tracked for 3 years, and medical record review
Enrollment • 46,206 telephone calls • 32,521 (70%) were households • 15,264 (47%) households screened for eligibility • 2964 (19% of households) contained an eligible subject. • 1841 (62% of those eligible) consented to participate. • 1463 completed the baseline interview and were randomized • 1175 (80.3% of those randomized) completed the study
Intervention and Usual Care • Intervention components • an individually and culturally tailored printed health guide • telephone counseling • Usual Care • Women in the control group received usual care from their provider, if any
Cost Estimation • Micro-costed the intervention • Variable cost: outreach worker forms (507 hours) • Fixed cost: Space, QA, Supplies • Costs were standardized to 2002 • Research costs were excluded
Effectiveness • Receipt of recent mammography and recent Pap smear (last 15 month). • Self report data • Accuracy of self report varied by race-ethnicity • McPhee SJ, Nguyen TT, Shema SJ, et al. Validation of recall of breast and cervical cancer screening by women in an ethnically diverse population. Prev Med. Nov 2002;35(5):463-473.
C1-C0 E1-E0 Cost Effectiveness Analysis • We calculated the incremental cost per woman screened Incremental Cost- Effectiveness Ratio =
Behavioral Interventions • General CEA framework holds, but caveats… • Behavior change is a “slow” process • Treat many to prevent a few • Use of intermediate outcomes (proxies)
Intermediate Outcomes • Outcome is clinically relevant and predicts mortality or morbidity • Receipt of a mammogram • Substance use abstinence • Change in dietary fiber • QALYs would require huge and/or very long studies
CEA with an Intermediate Outcome • Sufficient for publication • Hard to interpret ICER • Can’t easily compare two CEAs with different intermediate outcomes • Can’t compare CEA to other CEA from another clinical area • Sometimes only feasible approach
CEA with QALYs • Measure QALYs or • Translate intermediate outcome to QALYs • Either build a model de novo or use an existing model • Requires a lot of resources • Most useful, but most challenging
CEA and Behavior Change • “Getting the person to recognize that they have a problem is half the battle.” • Behavior change is a process, not a dichotomous outcome • Need to measure: • Starting point in the process • Movement in the process Wagner TH, Goldstein MK. Behavioral interventions and cost-effectiveness analysis. Prev Med 2004;39(6):1208-14.
Subgroup Analysis • Calculated cost-effectiveness ratios by baseline stage of change. • never • inconsistent (prior test, but not in last 15 months) • recent (prior test in last 15 months) • regular (prior test in last 15 months and another within two years of the last test).
Cost per Life Year Saved • Modified existing modelto assess cost per life year saved. • Only effects of mammography are included • Mandelblatt JS, Schechter CB, Yabroff KR, et al. (2004) Benefits and costs of interventions to improve breast cancer outcomes in African American women. J Clin Oncol. 22(13):2554-2566.
Summary • Incremental cost per woman screened • $436 per mammography • $380 per Pap smear • Cost per life year saved of $109,812->$500,000 • Low estimate= 1 “dose” • High estimate= repeats every two years • Annually > $1 million
Prior Research • Andersen et al (2002) much lower cost-effectiveness ratio, but effectiveness of intervention was not statistically significant. • Our intervention was highly effective (+7% more than Andersen)
Limitations • Cannot separate effect of health guide versus telephone counseling • No utility weights in model • Model only looks at mammography
Project 2: Abnormal Pap Smears • Highland Hospital (Oakland CA) routinely performs Pap smears in the ED • Low rates of follow-up among abnormal Pap smears (~30%)
Project 2 • Usual care: send the woman a letter if there is an abnormal Pap smear • This study evaluates the cost-effectiveness of usual care (a mailed postal reminder) with a tailored outreach intervention compared to usual care alone
Pap Abnormality • Atypical squamous cells of undetermined significance (ASCUS) • Atypical glandular cells of undetermined significance (AGUS) • Low-grade squamous intraepithelial lesion (LGSIL) • High-grade squamous intraepithelial lesion (HGSIL) Solomon D, Davey D, Kurman R, et al. The 2001 Bethesda System: terminology for reporting results of cervical cytology. JAMA 2002; 287:2114-9.
Methods • Eligibility • Abnormal Pap at Highland Hospital • Age 18-74 • English or Spanish speaking • Excluded • In process of follow-up • Pregnant and due after intervention period
Intervention • Randomized, controlled cohort trial • Two groups • Usual care: notified by telephone or mail, depending on the degree of abnormality • Usual care plus outreach and tailored individual counseling • Randomization without consent; 6-month rescue
Main Outcomes • Follow-up at 6 months • Costs • Incremental cost per follow-up
Costing • Micro-costed the intervention • Variable cost: outreach worker forms • Fixed cost: Space, QA, Supplies • We used payroll systems to identify outreach worker overhead costs
Break Even Analysis • 8% (n=29) had HGSIL (highest risk) • Intervention: 93% had follow-up • Control: 43% had follow-up
Conclusion • In this population, augmenting usual care with outreach and tailored individual counseling was relatively inexpensive and highly effective.