Download
1 / 53
530 likes | 552 Views
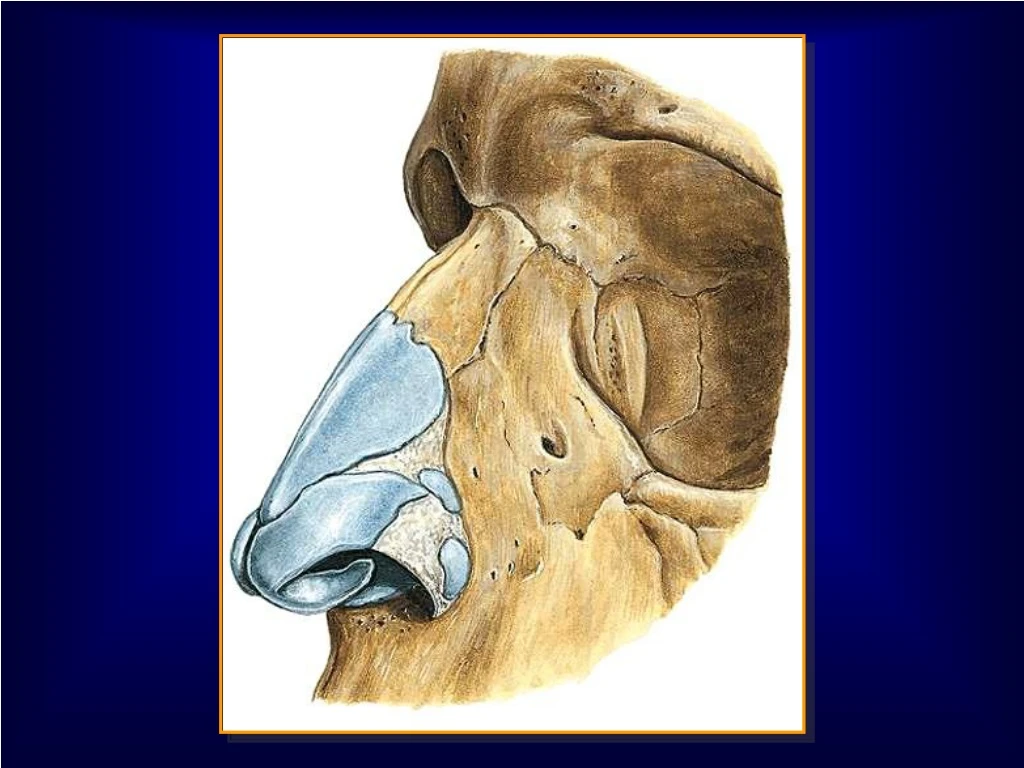
This schematic diagram illustrates the motion of a single cilium during the rapid forward beat and the slower recovery phase, as well as the cycle of events that leads to chronic rhinosinusitis. It highlights the ostial blockage, mucosal changes, damage to cilia and epithelium, stagnant secretions, bacterial growth, congestion, and infection in the sinus cavity.

E N D
Schematic diagram of motion of a single cilium during the rapid forward beat and the slower recovery phase.
Cycle of events that leads to chronic rhinosinusitis begins with ostial blockage Mucosal gas metabolism changes Secretions thicken; pH changes Cilia and epithelium are damaged Secretions stagnate Change in host milieu creates culture medium for bacterial growth in closed cavity Mucosal congestion or anatomic obstruction blocs airflow and drainage OSTIUM IS CLOSED Retained secretions cause tissue inflammation Mucosal thickening creates further blockage Bacterial infection develops in the sinus cavity
The expression sinusitis describes an inflammatory process present in the paranasal sinuses mucous membrane, due to disturbances of drainage and ventilation, as a result of infection, allergy or anatomical variations of the lateral nasal wall. This term refers to pathological changes present both in one sinus e. g. maxillary sinusitis and also in several paranasal sinuses (hemipansinusitis, pansinusitis).
For practical reasons in the daily clinical work both terms - sinusitis and rhinosinusitis are equivalent.
Two classifications of chronic rhinosinusitis are currently proposed in rhinological literature. The classification introduced by Kern in 1984 is based on the duration of the disease process and corresponding morphological changes in the mucosa of the sinuses: • Acute purulent rhinosinusitis - lasting up to 3 weeks, with one orseveral sinuses involved. • Subacute purulent rhinosinusitis - lasting up to 3 weeks to 3months.Morphological changes in the mucosa which occur withinthat time are usually reversible. • Chronic purulent rhinosinusitis - lasting over 3 months. This form ofthe disease process is thought to be a result of untreated orimproperly treated acute inflammation. Surgery to removeirreversibly changed mucosa is recommended.
The 1995 International Conference on Sinus Disease classification of rhinosinusitis is based on an assessment of the extent of pathophysiological processes involving the mucosa of the sinuses and the nasal cavity: • Acute rhinosinusitis is defined as an episodic inflammatoryprocess which does not leave any significant persistent damage ofthe mucosa after conservative treatment. • Acute recurrent rhinosinusitis refers to repeated episodes of acuteinflammation with complete recovery after conservativetreatment, causing no persistent damage of the mucosa. • Chronic rhinosinusitis is defined as persistent inflammation whichcannot be cured with conservative treatment.
The patient may complain of: • nasal blockage or congestion; • nasal discharge - serous, seropurulent,purulent; • postnasal discharge; • pain or pressure in the orbital region, pain orpressure in the region of the sinus affected by inflammation; • headache; • toothache.
Physical examination reveals: • oedema and reddening of the nasal cavities mucosa; • oedema of the skin in the region of the root of the nose and inthe region of the palpebras; • mucous, mucopurulent or purulent secretion in the nasal cavities; • mucous or purulent secretion in the nasopharynx; • purulent secretion on the lateral wall of the nasal cavity; • painfulness of the cheek when exerting pressure on the caninefossa (in the maxillary sinusitis) and when exerting pressure onthe upper wall of the orbit (in the frontal sinusitis).
Factors predisposing recurrences of acute rhinosinusitis Anatomic: • deviation of the nasal septum; • anatomical variations of the nasal lateral wall: • of the middle nasal concha, of the uncinate process, of the ridge of the nose, of the ethmoidal bulla, of the Haller’s cels; Morphological: • nasal polyps; • nasal tumours; • adenoids.
Factors predisposing recurrences of acute rhinosinusitis Oedemas of the mucosa: infection; allergy; rhinitis vasomotorica; rhinitis medicamentosa; hormonal disturbances. Traumas: local traumas; barotrauma; foreign bodies; iatrogenic. Constitutional: syndromes of ciliary disturbances; cystic fibrosis; immunological deficiencies.
The most often used antibiotics in the therapy of rhinosiusitis
Supplementary treatment • Decongestants should ensure restoration of the patency of theostio-meatal complex and thereby the sinuses ostia. • Mucolytic drugs act on the retained in the sinuses secretion in sucha way that it becomes more liquid thus easier to move. • Corticosteroids are recommended first of all in the therapy ofchronic inflammation. • Recommendation for the administration of antihistamines requirescomprehensive reasoning, because allergy plays a far smaller rolein the pathogenesis of rhinosinusitis than it is assumed.
Criteria for chronic rhinosinusitis In adults 8 weeks of persistent symptoms and sings or Four episodes per year of recurrent acute sinusitis, each lasting at least 10 days in association with Persistent changes on computer tomography 4 weeksafter medical therapy without intervening acute infection
Criteria for chronic rhinosinusitis In children 12 weeks of persistent symptoms and sings or: Six episodes per year of recurrent acute sinusitis, eachlasting at least 10 days in association with Persistent changes on computer tomography 4 weeksafter medical therapy without intervening acute infection
Criteria for chronic rhinosinusitis Symptoms and sings Adults and children Major Nasal congestion Nasal discharge Headache Facial pain or pressure Olfactory disturbance Minor Fever Halitiosis Children only Cough Irritability
The most often isolated microorganisms in rhinosiusitis Streptococcus pneumoniae Haemophilus influenzae Streptococcus pyogenes Staphylococcus aureus Anaerobes: Bacteroides Fusobacterium Peptostreptococcus Alpha- and beta-haemolytic streptococci Other Gram-negative bacterias