Download
1 / 26
260 likes | 270 Views
Explore the intricate anatomy of carotid arteries, their branches, and importance in cerebral circulation. Learn about indications and scanning protocols for Doppler imaging. Improve diagnostic accuracy and patient care.

E N D
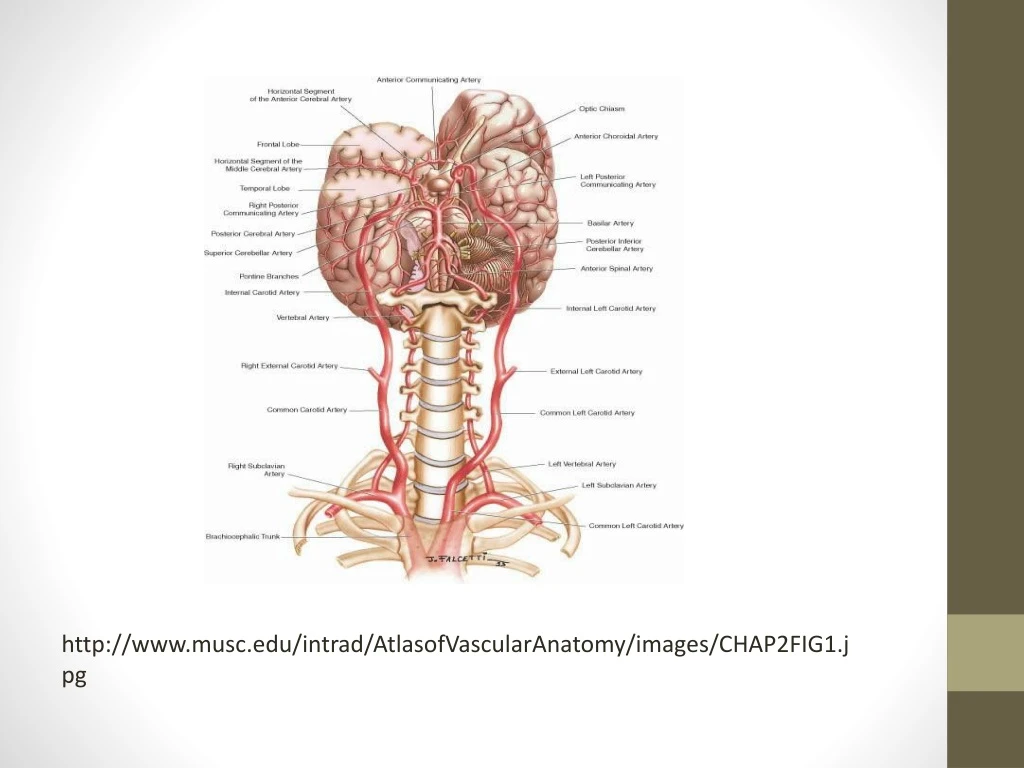
http://www.musc.edu/intrad/AtlasofVascularAnatomy/images/CHAP2FIG1.jpghttp://www.musc.edu/intrad/AtlasofVascularAnatomy/images/CHAP2FIG1.jpg
Normal Carotid artery bifurcation http:// www.specialistvascularclinic.com.au/ cv
Pictorial images showing normal common arteries and effect of the presence of plague http://www.nhlbi.nih.gov/health/health-topics/topics/cu/
ANATOMY Cerebrovascular The main arteries that supply the brain and the central nervous system are the Carotid (2)and vertebral (2) arteries running cephalad on both sides of the neck. These arise from the aortic arch. -On the right-the Brachiocephalic travels upwards and then branches into the right common carotid and subclavianarteries goes through at the upper border of the sterno-clavicular junction- supplies the brain and eyes-no extra cranial branches-intracranial segment consists of the petrous, the cavernous and the cerebral -On the left- the left common carotid artery(CCA) travels upward from the arch behindthe sterno-clavicularjoint There are no branches on either CCA. • CCAs divide into internal carotid arteries(ICA) and external carotid arteries(ECA), in mid cervical region at the upper border of the thyroid cartilage. • ECAs are superficial with eight branches- superior thyroid, the lingual, the external and internal maxillary,occipital, facial, and transverse facial, posterior auricular, superficial temporal arteries. The external carotid arteries do not supply the brain but becomes important collateral pathways in case of occlusion in the ICA and Vertebral arteries most vital to collateral circulation are those in communication with ophalmic artery and those that intercommunicate between muscular branches and the occipito-vertebral arteries
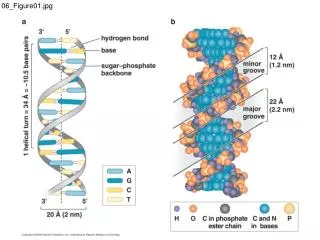
The left subclavian artery is the third major branch of the aortic arch The vertebral arteries arise off the subclavian arteries bilaterally, they ascend the neck along the right and left ICA, they lie within the foramina transverse sarium of the upper cervical vertebrae and winds and bends medially before entering the cranial cavity through the foramen magnum. The two arteries join to form the basilar artery The cerebral branches of the internal carotid arteries and vertebral arteries join at the base of the brain to form the circle of Willis The circle of Willis is a unique arrangement of vessels which provide a vital collateral network to maintain cerebral perfusion in the event of disease -anteriorly formed by the right and left `anterior cerebral arteries which are interconnected via the anterior communicating artery and posteriorly by the right and left posterior cerebral arteries, which are connected via the posterior communicating arteries .
INDICATIONS • -Transient I schaemic attacks • -Cerebro-vascular accident(CVA) • -AmaurosisFugax • Cervical bruit • -Neuralogical deficit-temporary or persisting • -Dizziness, Vertigo, headaches, fainting • Post operative surveillance • -Vertebral artery disease • -Follow up of previous noted disease
SCANNING PROTOCOL • The patient is scanned in supine position or erect sitting in a chair for patients with shortness of breath -elderly and obese-pronounced lordosis/curvatutre • Scanning all the arteries bilaterally • Common Carotid Arteries -Proximal and distal. • External Carotid Arteries - Proximal • Internal Carotid Arteries - Proximal, mid and distal • Vertebral- extra cranial- unless otherwise indicated for transntracranial imaging • CFD and B-mode • Transverse and long section of CCA and ICA bilaterally • Transverse and long section of the stenosis and bifurcation • Should include images showing the brachiocephalic, subclavian, • Spectral waveform in proximal ECA and proximal , mid and distal ICA • Spectral waveform in the vertebral artery bilaterally
Transcranial Doppler(TCD)/ Transcranialcolour Doppler(TCCD) -Four main windows Transtemporal. 2. Transorbital. 3.Sub Occipital. 4.Submandibular TRANSTEMPORAL -the following arteries are seen -Mid cerebral artery, at 35-60mm deep from the transducer –mean velocity of 62+/- 12 cm/s Anterior cerebral artery, at 60-75 mm deep from the transducer 50+/-11 cm/s mean velocity Posterior cerebral artery, at 65-75 mm deep from the transducer 39+/-10 cm/s Posterior communication artery, Anterior communication artery, 60-65mm depth from the transducer with a variation of mean velocities. Internal carotid artery Basilar artery ( posterior beam)
TRANSORBITAL -Ophthalmic artery - 45-65mm deep from the transducer 20+/-10cm/s -Internal carotid (siphon) artery 60-80 mm deep from the transducer -60-80mm deep from the transducer 47+/- 10 cm/s mean --velocity SUBOCCIPITAL Vertebral artery -50-85mm deep , 36+/-10 cm/s mean velocity SUBMANDIBULAR -Distal internal carotid artery, 35-70mm deep from the transducer, 39+/-10 cm/s mean velocity.
Indicatons for TCD orTCCD • Tight stenosis or occlusion of the ICA OR CCA • Presence of intracranial arterial disease • Transient ischaemic attacks with no other source of embolism • Vertebral artery disease • Arterial noise in the ear • Syncope or dizziness with head rotation • Monitoring cerebral perfusion in the intensive care unit after stroke ,subarachnoid haemorrhage or head injury • Studying changes in intracranial haemodynamics and emboli during carotid endarterectomy or coronary artery bypass grafting.
Transducer selection Selection of the protocol on the Duplex Doppler equipment should be –Vascular and specifically- carotid artery 3-9 MHz linear array – or curvilinear (when access to neck is limited e.g. in short neck, intravenous lines, or tracheotomy ties) transducer- to provide high resolution at a depth of 2-10cm Transducer footprint-rectangular-4-5cm long –narrow 1cm wide.
PATIENT’S HISTORY • Full history is undertaken – taking note of whether patient is • -hypertensive or has high cholesterol • -Diabetic • -Previous history of heart attach/ any intervention surgery like carotid endarterectomy, coronary bypass , stent placement or peripheral arterial revasculisation.
TECHNIQUE • Patient in supine position –neck extended ensure patient’s comfort • Neck exposure –maximized- rotating the neck away from side under examination • In B-mode and colour Doppler the Bracheo-cephalic and subclavian arteries examined noting any plague or calcification-noting any tortuosity of the vessels • The CCA is examined from proximal to distal in Longitudinal and transverse sections-looking at the wall outline for disease. • Survey the carotid bifurcation into ICA and ECA proximal, mid and distal • Tap the temporal bone to accurately identify the ECA- observe change in the waveform.
The ICA is examined from the bifurcation as far distally as possible- For transcranial scanning –use of windows mentioned above. The vertebral artery –examined with chin extended/flexed The colour box/sample volume is placed wide enough to get maximum information with the angle of isonation not more than 60degrees.
DIFFERENCIAL DIAGNOSIS • -Vertebral artery/vertebrobasilar disease • -Carotid artery dissection • -Carotid aneurysm • -Carotid body tumour • -MoyaMoya disease • -Takayasu’s arteritis • -Fibro muscular dysplasia
CRITEIA FOR DIAGNOSIS • Increase in mean velocity in the MCA • -120-150cm/s = minor stenosis • -150-200cm/s =moderate stenosis • ->200cm/s severe stenosis
NASCET CRITERIA Retrieved from: http://www.kup.at/journals/abbildungen/
Normal carotid artery spectral wave form Retrieved from: http://www.charlesbuntjer.com/chucks_research_projects_2007_12_14_carotid_arteries.htm
Carotid artery bifurcation Retrieved from: http://www.aultman.org/ourservices/Additional-Aultman-Programs-and-Services/additionalprogramsandservices/AultmanVascularServices/CarotidArteryUltrasound.aspx
Internal carotid artery demonstrating obstructing plague and colourdoppler aliasing Retrieved from: http://www.bobblum.com/ESSAYS/BIOMED/Coronary-CT.html
High resistance common carotid artery Retrieved from: http://www.angiologist.com/arterial-disease/carotid-artery-occlusion/
Vertebral artery http://sonoscapeportableultrasound.com/wp-content/uploads/2011/07/Vas.Vertebral-artery.CD_.jpg
Normal vertebral artery http://www.ultrasoundpaedia.com/uploads/53003/ufiles/vascular/carotids/vert-dopp-norm.jpg
References • Nascet criteria image retrieved from: http://www.kup.at/journals/abbildungen/ • Normal carotid artery image retrieved from: http://www.charlesbuntjer.com/chucks_research_projects_2007_12_14_carotid_arteries.htm • Carotid artery bifurcation image retrieved from:http://www.aultman.org/ourservices/Additional-Aultman-Programs-and-Services/additionalprogramsandservices/AultmanVascularServices/CarotidArteryUltrasound.aspx • Internal carotid artery image retrieved from:http://www.bobblum.com/ESSAYS/BIOMED/Coronary-CT.html • High resistance common carotid artery image retrieved from:http://www.angiologist.com/arterial-disease/carotid-artery-occlusion/
References Hamper, M.U., M.R. DeJong, and L.M. Scoutt. 2007. Ultrasound evaluation of the lower extremity veins. Radiologic Clinics of North America 45: 525-545. • Kupinski, A.M. 2013. Diagnostic medical sonography. The vascular system. Philadelphia: J.K. Stegman3 • Myers, K.A and A. Clough. 2004. Making sense of vascular ultrasound a hands on guide. London: Arnold • Zwiebel, W.J., and J. Pellerito. 2005. Introduction to Vascular Ultrasound. 5th ed. Philadelphia: W.B. Sanders