Download
1 / 25
250 likes | 629 Views
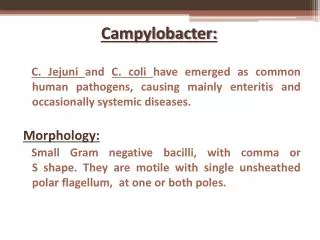
Campylobacter Enteritis. Summer, 2010 SW Montana County Health Departments Allison McIntosh, PhD Student Walden University PubH 8165-1 Instructor: Dr. Howard Rubin. Purpose of Presentation.

E N D
Campylobacter Enteritis Summer, 2010 SW Montana County Health Departments Allison McIntosh, PhD Student Walden University PubH 8165-1 Instructor: Dr. Howard Rubin
Purpose of Presentation To exchange knowledge of the transmission, recognition, reporting of, treatment, and prevention of Campylobacter enteritis in Southwest Montana.
Agenda • Discuss terminology • Prevalence • Routes of exposure • Reporting procedure • Treatment • Prevention
Learning Objectives: By the end of the session participants will: • Define campylobacter and enteritis • List three routes of exposure to campylobacter • Identify an example of a food borne transmission and a water borne transmission • List the main two symptoms of campylobacter • Explain the reporting procedure in Montana • List one treatment option for campylobacter • List two complications of Campylobacter enteritis • Expand on ways to avoid cross contamination and list two ways to prevent campylobacter
Picture of Campylobacter jejuniPublic Health Image Library (2010). Campylobacter. Image 5781. Retrieved July 15, 2010 from http://phil.cdc.gov/phil/quicksearch.asp
So what is enteritis? • Inflammation of the small intestine. Causes: • Eating or drinking substances that are contaminated with bacteria (in this case Campylobacter jejuni). • RESULTS IN: inflammation and swelling, which may lead to pain, cramping, diarrhea, fever, and dehydration. MedLine Plus (2010). Enteritis. Retrieved July 10, 2010 from http://www.nlm.nih.gov/medlineplus/ency/article/001149.htm
Prevalence • 2008 in Montana: 14.9 cases per 100,000 population per year • May to August are the most common months when 49% of all infections occurred Communicable Disease Stats and Facts (2008). Annual report. Retrieved July 18, 2010 from http://www.dphhs.mt.gov/PHSD/epidemiology/documents/AnnualReport2008FINAL_03_31_2010.pdf • Nationwide there are an estimated 2.5 million cases (Alterkruse, Stern, Fields, & Swerdlow, 1999)
Routes of Exposure • Food-borne: eating meat or drinking milk of infected animals • Cross-contamination: from cooking utensils such as a raw chicken placed on a cutting board and then using the board to prepare other food • Water-borne: Drinking un-chlorinated waters • Fecal-oral: Feces of infected animals are introduced to the oral cavity from poor hand hygiene
Food-borne Gastroenteritis from confirmed campylobacter Australian study: Population risk factors • Eating cooked and/or undercooked chicken (29.3%) • Barbequed meats placed on plate used for raw meat • Around domestic chickens less than 6 month old • Around dogs less than 6 months old • Having a gastrointestinal condition, liver disease, or being immuno-compromised from drugs Stafford, R..J., Schluster, P.J., Wilson, A.J., Kirk, M.D., Hall, G., Unicomb, L. (2008). Population-attributable risk estimates for risk factors associated with campylobacter infection, Australia. Emerging Infectious Disease (4)6, 895-901. Retrieved July 18, 2010 from http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2600281/pdf/07-1008_finalR.pdf
Waterborne Outbreaks • Summer 1981, Colorado, drinking water for campers (Hopkins, Olmstead, & Istre (1984). • Summertime camping trip, Grand Teton Park, WY, untreated surface water (Taylor, Brown, & McDermott, 1982). • Outdoor infantry drill in Utti, Finland, untreated surface water (Aho, Kurki, Rautlin, & Kosunen, (1989). • Sweden, communal tap water (Martin, Penttinen, Hedin, Ljungstrom, Allestam, Andersson, & Giesecke (2006)
Characteristics of the illness • Incubation 24 to 72 hours but may be a week if small amounts of bacteria are ingested • Prodromal syptoms: nonspecific-headache, muscle pain, chills, fever) • Hallmark symptom: DIARRHEA, watery stools, 8 or more in a day, may turn bloody • Abdominal pain may be like appendicitis • The peak of the illness lasts 24 to 48 hours and usually resolves in a week Blaser, M.J. (1997). Epidemiologic and clinical features of Campylobacter jejuni infection. Journal of Infectious Disease, 176 (SuppS), S103-S105. Available at http://www.cdc.gov/ncidod/eid/vol5no1/altekruse.htm
Serious but Rare • Guillain-Barré syndrome (GBS) • Reiter syndrome • Both GBS and Reiter syndrome are thought to be autoimmune responses stimulated by infection. Altekruse, S.F., Stern, N.J., Fields, P.I., Swerdlow, D.L. (1999). Campylobacter jejuni- An emerging foodborne pathogen. Emerging Infectious Disease, 5(1), Retrieved july 18, 2010 from http://www.cdc.gov/ncidod/eid/vol5no1/altekruse.htm
Costs Associated with Guillain-Barré syndrome • Of an estimated 2,628 to 9,575 new U.S. cases with GBS annually, 526 to 3,830 are triggered by infection with Campylobacter. Reducing Campylobacter in food could prevent up to $5.6 billion in costs annually. Buzby, J.C., Roberts, T., Allos, B.M.(1997). Estimated annual costs of Campylobacter associated Guillain-Barre Syndrom. Agricultural Economic Report No. (AER 756). USDA, Economic Research Service. Retrived July 3, 2010 from http://www.ers.usda.gov/Publications/AER756/
Reporting procedure ). Clinical description • An infection that may result in diarrheal illness of variable severity Laboratory criteria for diagnosis • Isolation of Campylobacter from any clinical specimen (stool culture) Case classification • Probable: a clinically compatible case that is epidemiologically linked to a confirmed case • Confirmed: a case that is laboratory confirmed Only confirmed cases are reported to the laboratory-based surveillance system managed by the Foodborne and Diarrheal Diseases Branch, Division of Bacterial and Mycotic Diseases, National Center for Infectious Diseases, CDC. Case Definitions for Infectious Conditions Under Public Health Surveillance [MMWR 1997;46(RR10)] (available at http://www.cdc.gov/mmwr/preview/mmwrhtml/00047449.htm
Treatment • Usually cases resolve on their own. • Potential for dehydration: May need replacement intraveneously or by oral route • If symptoms progress treat with Erythromycin or ciprofloxacin (Blaser, 1997) • Resistant strains are increasing with both animals as hosts and also humans (Judicious Use, 2001). • Seek medical care for bloody diarrhea and fever over 101 degrees (Javid & Ahmed, 2009)
Control of Campylobacter spread through the Food Safety and Inspection Service of the USDA On the farm: • The USDA recommends good sanitary practices to help control the spread among farm animals and birds • Pasteurization of milk and dairy products • Treatment/testing of municipal water supplies In the plant: At Plants: • Recommendations on how to handle raw (non-sterile) foods where up to 50 to 80% of poultry carry campylobacter At retail: • Voluntary food recalls by distributors USDA (2006). Foodborne Illness and Disease. Retrieved July 18, 2010 from http://www.fsis.usda.gov/factsheets/Campylobacter_Questions_and_Answers/index.asp
Prevention of Campylobacter exposure for consumers • Freezing poultry in home freezers generally not cold enough to kill natural bacteria in poultry • CLEAN: Wash Hands and Surfaces Often • Wash your hands with warm soapy water • Wash utensils, cutting boards, dishes, and countertops • Paper towels may be more safe USDA (2006). Foodborne Illness and Disease. Retrieved July 18, 2010 from http://www.fsis.usda.gov/factsheets/Campylobacter_Questions_and_Answers/index.asp
Separate food items • Keep raw chicken and meat separate in the shopping cart and refrigerator • It is recommended that it may be a good investment to use one cutting board for raw meats and one for fresh vegetables USDA (2006). Foodborne Illness and Disease. Retrieved July 18, 2010 from http://www.fsis.usda.gov/factsheets/Campylobacter_Questions_and_Answers/index.asp
Food Safety • Cook all meats and poultry and leftovers to 160 to 165 degrees • Refrigerate leftovers promptly • Cool quickly, place in shallow bowl so that food cools before placing in refrigerator USDA (2006). Foodborne Illness and Disease. Retrieved July 18, 2010 from http://www.fsis.usda.gov/factsheets/Campylobacter_Questions_and_Answers/index.asp
Learning Objectives: By the end of the session participants will: • Define campylobacter and enteritis • List three routes of exposure to campylobacter • Identify an example of a food borne transmission and a water borne transmission • List the main two symptoms of campylobacter • Explain the reporting procedure in Montana • List one treatment option for campylobacter • List two complications of Campylobacter enteritis • Expand on ways to avoid cross contamination and list two ways to prevent campylobacter
TO Sum Up • Campylobacter enteritis may be even more common than we know • There are potential serious conditions which may result with campylobacter infections • Immuno-suppressed patients are expected to increase with our aging population and so rates of serious infections may go upmaking them more susceptible • There are concerns about antibiotic resistant strains of Campylobacter and Salmonella which could result in a crisis • Montana has possibly more of a potential for water-borne campylobacter exposure because of the popularity of recreation in the back-country with untreated water. • Campylobacter enteritis is a reportable disease in Montana
References Aho, M., Kurkis, M., Tautelin, H., Kosunen, T.U. (1989). Waterborne outbreak of Campylobacter enteritis after outdoors infantry drill in Utti, Finland. Epidemiology of Infections, 103, 133-141. Retrieved July 1, 2010 from http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2249494/pdf/epidinfect00016-0137.pdf Altekruse, S.F., Stern, N.J., Fields, P.I., Swerdlow, D.L. (1999). Campylobacter jejuni- An emerging foodborne pathogen. Emerging Infectious Disease, 5(1), Retrieved july 18, 2010 from http://www.cdc.gov/ncidod/eid/vol5no1/altekruse.htm Bad Bug Book (2009). Foodborne pathogenic microorganisms and natural toxins handbook: Campylobacter jejuni. U.S. Food and Drug Administration. Retrieved July 1, 2010 from Public Health Image Library (2010). Campylobacter. Image 5781. Retrieved July 15, 2010 from http://phil.cdc.gov/phil/quicksearch.asp Blaser, M.J. (1997). Epidemiologic and clinical features of Campylobacter jejuni infection. Journal of Infectious Disease, 176 (SuppS), S103-S105. Available at http://www.cdc.gov/ncidod/eid/vol5no1/altekruse.htm .
References Buzby, J.C., Roberts, T., Allos, B.M.(1997). Estimated annual costs of Campylobacter associated Guillain-Barre Syndrom. Agricultural Economic Report No. (AER 756). USDA, Economic Research Service. Retrived July 3, 2010 from http://www.ers.usda.gov/Publications/AER756 Case Definitions for Infectious Conditions Under Public Health Surveillance [MMWR 1997;46(RR10)] (available at http://www.cdc.gov/mmwr/preview/mmwrhtml/00047449.htm Communicable Disease Summary ( 2008). Montana Department of Public Health and Human Services. Retrieved June 28, 2008 from http://www.dphhs.mt.gov/PHSD/Communicable-disease/documents/2008stats.pdf Communicable Disease Stats and Facts (2008). Annual report. Retrieved July 18, 2010 from http://www.dphhs.mt.gov/PHSD/epidemiology/documents/AnnualReport2008FINAL_03_31_2010.pdf
References Hopkins, R.S., Olmstead, R., & Istre, G.R. (1984). Endemic Campulobacter jejuni infection in Colorad: identified risk factors. American Journal of Public Health , 74, 249-250. Javid, M.H. & Ahmed, S.H. (2009). Campylobacter Infections: Treatment and Mediction. eMedicine. Retrieved July 5, 2010 from http://emedicine.medscape.com/article/213720-treatment Judicious Use of Antimicrobials for Poultry Veterinarians (2009). The Food and Drug Administration, Center for Veterinary Medicine., 1-13. Martin, S., Penttinin, P., Hedin, G., Ljungstrom M., Allesam, G. Anderson, Y., Giesecke, J. (2006). A case-control study to investigate concomitant waterborne outbreaks of Campylobacter and gastroenteritis in Sweden, 2002-2003. Retrieved June 19, 2010 from http://www.iwaponline.com/jwh/004/0417/0040417.pdf MedLine Plus (2010). Enteritis. Retrieved July 10, 2010 from http://www.nlm.nih.gov/medlineplus/ency/article/001149.htm
References Public Health Image Library (2010). Campylobacter. Image 5781. Retrieved July 15, 2010 from http://phil.cdc.gov/phil/quicksearch.asp Stafford, R..J., Schluster, P.J., Wilson, A.J., Kirk, M.D., Hall, G., Unicomb, L. (2008). Population-attributable risk estimates for risk factors associated with campylobacter infection, Australia. Emerging Infectious Disease (4)6, 895-901. Retrieved July 18, 2010 from http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2600281/pdf/07-1008_finalR.pdf Taylor, D.N., Brown, M., McDermott, K.T. (1982). Waterborne transmission of Campylobacter enteritis. Microbial Ecology, 8, 347-354. USDA (2006). Foodborne Illness and Disease. Retrieved July 18, 2010 from http://www.fsis.usda.gov/factsheets/Campylobacter_Questions_and_Answers/index.asp