Download
1 / 22
220 likes | 236 Views
Explore the population-based impact of antiretroviral treatment (ART) in regions with high HIV prevalence, highlighting ART coverage, mortality reductions, MTCT rates, employment recovery, and implications of HIV-related aging on the population.

E N D
Population-based impact of ART in high HIV prevalence settings Marie-Louise Newell Professor of Global Health Faculty of Medicine, Faculty of Social and Human Sciences, University of Southampton USRG Population Health Summer Conference June 2014
Estimated number of Adults and Children living with HIV by region, 2012 Eastern Europe & Central Asia 1.3 million [1.0 – 1.7 million] Western & Central Europe 860 000 [800 000 – 930 000] North America 1.3 million [980 000 – 1.9 million] East Asia 880 000 [650 000 – 1.2 million] Middle East&North Africa 260 000 [200 000 – 380 000] Caribbean 250 000 [220 000 – 280 000] South & South-East Asia 3.9 million [2.9 – 5.2 million] Sub-Saharan Africa 25.0 million [23.5 – 26.6 million] Latin America 1.5 million [1.2 – 1.9 million] Oceania 51 000 [43 000 – 59 000] Total: 35.3 million (32.2 – 38.8 million) Source: UNAIDS 2013 report
New infections and AIDS deaths 2012 Estimated number of people newly infected with HIV: Estimated number of AIDS deaths: About 2/3 of all people with HIV globally reside in sub-Saharan Africa Source: UNAIDS 2013
Global antiretroviral treatment (ART) programme scale-up • In 2012 there were nearly 10m HIV infected people on ART globally, of whom 7.5 million (~ 25% of the estimated HIV infected population) in sub-Saharan Africa • 1.6m more people were receiving ART in low- and middle-income countries in 2012 than in 2011, most of this increase came from sub-Saharan Africa • South Africa has the largest absolute number of HIV infected people, ~6.4m, worldwide and the largest number on ART at > 2m in 2012
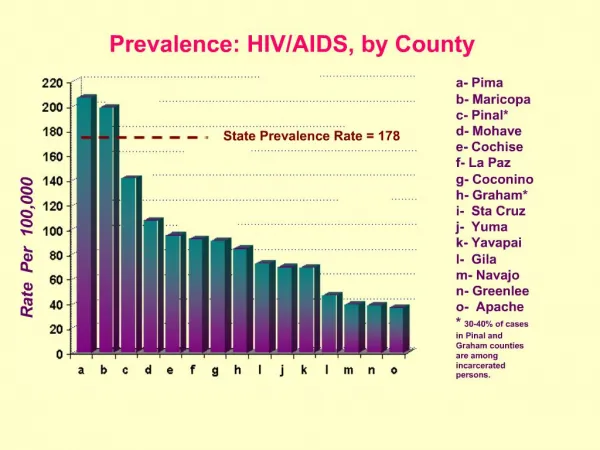
HIV prevalence,ART coverage, and HIV incidence in the population
Africa Centre surveillance area HIV prevalence 2004-2011 Females • In 2011, overall HIV prevalence among adults ≥ 15 years of age was 24% • Among 15-49 year residents, prevalence increased from 21% in 2004 to 29% in 2011; • ART coverage of HIV infected people in this age group increased from 0% in 2004 to nearly 31% in 2011 Zaidi et al, AIDS 2013 Males Red HIV prevalence; Blue ART coverage
HIV incidence by age and sex, 2004-2011, residents in Africa Centre surveillance area Females Males HIV incidence overall about 3%; peaking at 7% at age 24 for women and nearly 5% in men at age 29 Tanser, Bärnighausen, Grapsa, Zaidi & Newell, Science 2013
ART coverage 2004-112004-2011 • ART coverage = proportion of the total HIV-infected population receiving ART • Patients on treatment: Individual, geo-located DOH programme adult patients actively on treatment in June (2004-2011) • HIV-infected: Individual, geo-located, HIV positive adults identified through population-based HIV surveillance data (2004-2011) *Using a standard Gaussian kernel of radius 3km
Adjusted HIV acquisition hazard by ART coverage category Adjusted for age, sex, community-level HIV prevalence, urban vs. rural locale, marital status, >1 partner in last 12 months, and household wealth index Tanser et al, Science, 2013
Mother-to-child transmission • Identification of HIV in early pregnancy • ART from the 2nd trimester of pregnancy, during delivery and breastfeeding • Substantial and significant reduction of MTCT rates, from about 15% to <2% at 6 weeks and 30% to <4% at 18 months
Mortality (deaths per 10,000 pyo) in the 0-4 year age group; 2000-2009
Child mortality and association with PMTCT and ART roll-out • Under- 2 child mortality rates in the surveillance area declined substantially from 2001: • sdNVP PMTCT availability associated with a non-significant 15% decrease, • ART roll-out associated with a 34%-55% reduction (depending on estimated coverage in setting) (Ndirangu et al AIDS 2010, 24: 593-602) • Subsequently, with linked ART data, we showed that under-5 mortality in children of HIV infected mothers on ART and those born to uninfected mothers did not differ significantly (Ndirangu et al, Antiviral Therapy 2012; 17: 81-90)
Mortality in adults 2000-2009, deaths per 10,000 PYO 50-64 yr Age Standardised 15-49 yr Age Standardised Herbst et al; Population Health Metrics 2011
Mortality reductions lead to major gains in life expectancy 60.5 years in 2011 49.2 years in 2003 Bor, et al. Science 2013; 339: 961-965
Employment recovery following ART initiation In this high unemployment area, the likelihood of being in employment further decreases with HIV disease progression. However, within 3-4 years following ART initiation employment likelihood is back to ‘normal’ levels Bor, Tanser, Newell, Bärnighausen Health Affairs 2012
Aging of the population Aging of the population as HIV infected people on treatment live longer, with continued low level HIV incidence in the over-50s: • HIV prevalence in people aged over 50 years will nearly double by 2040 • The fraction of HIV-infected people over 50 years will triple in the same period • in 2011 about 1:7 HIV infected people were 50 years or older, in 2040 this will be 1:4 Hontelez et al, AIDS 2011; 25(13): 1665-7 Walker et al Lancet Global Health 2013; 1: e282-288
Elimination of the HIV epidemic? • Results from a trial of ART in discordant couples have strengthened the arguments for Treatment-as-Prevention, with statistical models suggesting possible elimination of HIV from the population (Cohen et al NEJM 2011; 365: 493-505) • Recent models suggest that high ART coverage at CD4 <350 cells/µl together with male medical circumcision would be most cost-effective in reducing transmission and mortality (Bärnighausen, Bloom and Humair, PNAS 2012; 109: 21271-76) • High ART coverage at eligibility of CD4 < 350 cells/µl is modelled to virtually eliminate HIV albeit up to 10 years later than universal ART would (Hontelez et al. PLoS Med 2013)
Conclusion • HIV continues to be a major public health challenge in sub-Saharan Africa • Impressive increase in number of HIV infected people on treatment • Substantial reduction in new infections is possible • Mother-to-Child transmission can be ‘virtually’ eliminated • Sexual transmission can be reduced significantly • Reduction in HIV-related mortality and consequent aging of the population will necessitate refocussing of health care programmes