Download
1 / 31
310 likes | 453 Views
Use of Marginal Structural Models in a Comparative Effectiveness Study of Intravenous Iron Formulations in End-Stage Renal Disease. M. Alan Brookhart , Ph.D. Department of Epidemiology, UNC Gillings School of Global Public Health University of North Carolina at Chapel Hill. Overview.

E N D
Use of Marginal Structural Models in a Comparative Effectiveness Study of Intravenous Iron Formulations in End-Stage Renal Disease M. Alan Brookhart, Ph.D. Department of Epidemiology, UNC Gillings School of Global Public Health University of North Carolina at Chapel Hill
Overview • End-stage renal disease and anemia management • Overview of my ARRA-funded CER study of iron • Use of MSMs to estimate long-terms effects of iron
Conflict of Interest / Acknowledgments • Project is supported by a contract from AHRQ’sDEcIDE center • I have received research support from Amgen (that placed no restrictions on publications) and have sat on advisory boards for Amgen and Pfizer (honorarium declined or paid to institution).
End-Stage Renal Disease • 50% have diabetes • 85% have hypertension • 27% have ischemic heart disease • 2 major hospitalizations /year • 20-25% annual mortality rate 2006 USRDS Annual Data Report
Anemia is a common complication of ESRD • Anemia = low hemoglobin/hematocrit levels • Anemia leads to • Cardiovascular problems • Decreased energy level, cognitive and physical functioning • Requires transfusions • In ESRD, anemia caused by lack of erythropoietin and exacerbated by loss of iron
Anemia Management • RCTs have shown that treatment with recombinant erythropoietin (EPO) and intravenous iron raises hematocrit in ESRD • In widespread use in ESRD population • Controversy: • Cost: • Medicare spent over $2B on EPO in 2005 • EPO has been a major source of revenue for dialysis centers • Safety: • Questions about safety of EPO, appropriate hematocrit targets • 2007 FDA placed a “black box” advisory on the label of ESAs (EPO) • > increased use of iron for anemia management
Trends in Iron Dosing in US Hemodialysis Patients(by formulation and overall)
Potential Benefits and Risks Associated with IV Iron Use • Aggressive use of iron may safely treat anemia, reduce need for EPO (DRIVE study) • But may increase risk of iron overload, infections or other adverse outcomes
Comparative Effectiveness of Intravenous Iron in End-Stage Renal Disease • 3-year project funded through AHRQ • Co-investigators: • AbhiKshirsagar, MD – UNC Kidney Center • Steve Cole, PhD – UNC Epidemiology • TilSturmer, MD – UNC Epidemiology • Wolfgang Winkelmayer, MD — Stanford Medicine
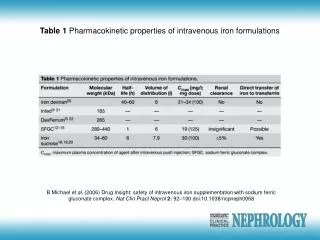
Evidence Gap 1: Investigate the CER of different iron formulations • Two formulations in widespread use • Ferric gluconate • Iron sucrose • Different pharmacologically • Little data on comparative effectiveness
Evidence Gap 2: Investigate the CER of iron dosing approaches • Iron status measured with monthly labs • Transferrin saturation • Ferritin • When should iron be administered? • How should it be administered? • Maintenance dosing versus bolusdosing • How much should be administered?
DaVita Data • Large dialysis provider in the US • 1,500 units and 150,000 patients • Data from 2004-2009 on 250,000 patients • Labs every 2 weeks to month • Individual treatment • Clinical data: BP, BMI, vascular access in use
Renal Research Institute Data • Small chain of dialysis providers associated with academic medical centers in the US • 15,000 prevalent patients • Similar clinical data to DaVita • Quality of life (SF-36), recorded every three weeks • Additional labs: C-reactive protein
Medicare Data • Hospitalization data • Data from physicians, dialysis encounters outside of DaVita • Date and cause of death • Transplant information • Linked with DaVita and RRI data
Outcomes • Anemia management outcomes • Decreased use of ESAs • Hemoglobin control • Quality of Life • Infection • Sepsis, vascular access infection, infection-related mortality • Cardiovascular • AMI, stroke, CV-related mortality • Hypersensitivity: Anaphylaxis, drug allergy • All-cause mortality
Aim 1: Comparative Study of Acute Effects Rapid onset iron exposure effects (Case-Crossover Analysis) Event of interest: anaphylaxis, hospitalization for sepsis, AMI • Examine effects on clinical outcomes that occur within days after exposure to iron • Case crossover design analyzed by conditional logistic regression • Contrasts of Interest • Iron sucrose versus ferric gluconate • High dose versus low dose start of dialysis Control Period Hazard Period X
Aim 1: Strengths and Limitations • Strengths of case crossover design • Self-controlled, not confounded by time-invariant covariates • Limitations • Confounded by time-varying confounders • Hospitalizations • Sensitivity analysis • control for hospitalization status • vary size of hazard and control windows
Aim 2: Comparative Study of Short-Term Effects Study Design For Intermediate-term Effects (ITT Analysis, with Propensity Score Adjustment) • Examine effects that occur within 6-months after exposure to iron • Propensity score/IPTW to adjust for confounders • Compare risk of • Iron sucrose versus ferric gluconate • High dose versus low dose • Compare bolus versus maintenance Clinical outcome 3-month rhEPO, TSAT, Ferritin assessment Censoring 6-month baseline period: covariates defined 1-month iron exposure assessment X O First TSAT lab, at least 6 months of after the start of dialysis 3-month follow-up period
Aim 2: Strengths and Limitations • Strengths of IPTW, propensity score analysis • Control for many confounders • Yields interpretable causal effect • Limitations • Violations of non-positivity • Up-weighting of patients with rare treatment or data errors • Unmeasured confounders • Sensitivity analysis • Use SMR-weighting • Vary definitions of high versus low dose
Aim 3: Heterogeneity of Short-Term Effects • Repeat aim 2 across a range of clinically-relevant subgroups • Iron status (high ferritin, low Tsat) • Liver disease • Diabetes • Inflammation • Cause of end-stage renal disease • Age • History of infection
Aim 4: Comparative Study of Chronic Effects Chronic Effects (Marginal Structural Model) • Examine outcomes caused by long-term exposure • Iron exposure is a longitudinal variable • Compare risk of • Continual treatment with iron sucrose versus ferric gluconate Time 1 Time 2 … Time n Censoring 6-month baseline period: covariates defined 1-month iron exposure assessment 1-month iron exposure assessment 1-month iron exposure assessment O First TSAT lab, at least 6 months of after the start of dialysis 1-month covariate & outcome assessment 1-month covariate & outcome assessment 1-month covariate & outcome assessment
Time Dependant Confounding Iron Treatment at Month 1 Iron Treatment at Month 2 Outcome Ferritin, TSat, Infection status Ferritin, TSat, Infection status
Marginal Structural Model Analysis • Marginal structural model to address time-varying confounders • Causal contrasts of interest • Continual treatment with iron sucrose versus ferric gluconate • Continual treatment with high versus low dose • Two-stage treatment model • for treatment versus no treatment • high dose versus low dose • Assume formulation choice is exogenous
Issue 1: A month is a long time for a dialysis patient • Dialysis patients have very dynamic health status • Iron exposure during the month may be dependant on events occurring during the month • Tangles up effect of events with effect of iron • Possible solution: • Unit of observation is a one-week period of event the dialysis session?
Issue 2: Causal Contrast • In this setting, MSMs returns an effect estimate that is not directly clinically relevant • E.g., effect of continuous treatment with high dose versus continuous treatment with low dose • Better approach would use a dynamic treatment approach, compare the effect of treat with 1g of iron when Tsat<20% versus Tsat<15%. • Standard MSM could reveal risks of chronic treatment • Iron is not given in this way, are data informative about such treatment effects?
Issue 3: Non-Positivity • Iron treatment decisions driven strongly by transferrin saturation and infection status • Some patients almost always treated, some almost always untreated • Treatment contrary to prediction/indication can lead to lead to huge weights • Data errors can also lead to very large weights • We will experiment with weight truncation and trimming
Expected Results, Problems, Future Directions • Multiple analytic methods and sensitivity analysis provides robustness to finding • If methods do not agree, have to decide why • Estimating different causal effects • Assumptions hold for one method but not another • Expect the study will yield important evidence about the comparative effectiveness of different iron formulations and different dosing regimens • Future work with dynamic treatment models may help to identify “treatment strategies” to minimize risk and maximize clinical benefit of anemia management RCTs
“Black Box” Warning • On March 9th, 2007 FDA added a “black box” warning to labels of all ESA. “The new boxed warning advises physicians to monitor red blood cell levels (hemoglobin) and to adjust the ESA dose to maintain the lowest hemoglobin level needed to avoid the need for blood transfusions. Physicians and patients should carefully weigh the risks of ESAs against transfusion risks.”