Download
1 / 1
10 likes | 302 Views
발달장애인 의료실비보험 예약가입 신청서. 국내 유일 발달장애인 의료실비보험 출시 !. 계약자 ( 부양자 ) : 주민등록번호 : 피보험자 : 주민등록번호 : 주 소 : 장애유형 : ( ) 급

E N D
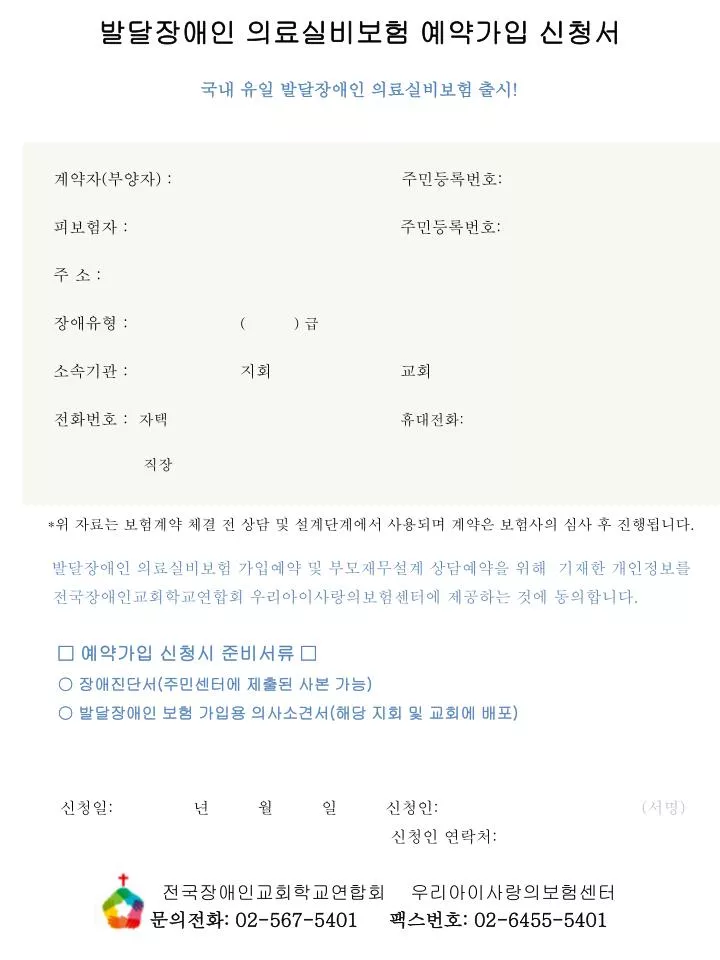
발달장애인 의료실비보험 예약가입 신청서 국내 유일 발달장애인 의료실비보험 출시! 계약자(부양자) : 주민등록번호: 피보험자 : 주민등록번호: 주 소 : 장애유형 :( ) 급 소속기관 : 지회 교회 전화번호 :자택 휴대전화: 직장 *위 자료는 보험계약 체결 전 상담 및 설계단계에서 사용되며 계약은 보험사의 심사 후 진행됩니다. 발달장애인 의료실비보험 가입예약 및 부모재무설계 상담예약을 위해 기재한 개인정보를 전국장애인교회학교연합회 우리아이사랑의보험센터에 제공하는 것에 동의합니다. • □ 예약가입 신청시 준비서류 □ • ○장애진단서(주민센터에 제출된 사본 가능) • ○ 발달장애인 보험 가입용 의사소견서(해당 지회 및 교회에 배포) 신청일: 년 월 일 신청인:(서명) 신청인 연락처: 전국장애인교회학교연합회 우리아이사랑의보험센터 문의전화: 02-567-5401 팩스번호: 02-6455-5401
