Download
1 / 35
540 likes | 1.3k Views
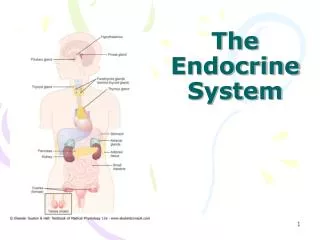
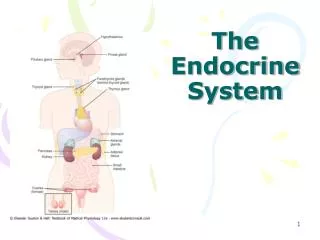
Multiple Endocrine Neoplasia MEN I/MEN II. Todd A. Nickloes, DO, FACOS, FACS Associate Professor Division of Trauma/Critical Care Department of Surgery University of Tennessee Medical Center-Knoxville. MEN I Involves the 3 P’s Pituitary Parathyroid Pancreatic islet cells MEN II

E N D
Multiple Endocrine Neoplasia MEN I/MEN II Todd A. Nickloes, DO, FACOS, FACS Associate Professor Division of Trauma/Critical Care Department of Surgery University of Tennessee Medical Center-Knoxville
MEN I • Involves the 3 P’s • Pituitary • Parathyroid • Pancreatic islet cells • MEN II • MEN II-A • Medullary carcinoma of thyroid • Pheochromocytoma • Parathyroid hyperplasia • MEN II-B • Medullary carcinoma of thyroid • Pheochromocytoma • Ganglioneuromatosis (mucosal neuromas) • Marfanoidhabitus MEN I/MEN II
MEN I • Involves the 3 P’s • Pituitary • Parathyroid • Pancreatic islet cells • MEN II • MEN II-A • Medullary carcinoma of thyroid • Pheochromocytoma • Parathyroid hyperplasia • MEN II-B • Medullary carcinoma of thyroid • Pheochromocytoma • Ganglioneuromatosis (mucosal neuromas) • Marfanoidhabitus MEN I/MEN II
MEN I • Involves the 3 P’s • Pituitary • Parathyroid • Pancreatic islet cells MEN I
Parathyroid • Hyperparathyroidism occurs in over 90% of pts. • Typically first detectable abnormality • Nephrolithiasis/Hypercalcemia • Usual presentation: • 25-35 y/o presents with predominantly urinary complaints • Nephrolithiasis • Polyuria • Hypercalcemia • Muscle weakness • Anorexia/Nausea • Not as in primary hyperparathyroidism (more on this later) • Postmenopausal women • Nephrolithiasis • Hypertension • Osteoporosis • Emotional disturbances MEN I
Parathyroid • This is a multi-glandular process • Diffuse hyperplasia • Metachronous development of multiple adenomas • 4 gland enlargement • Not as in primary HPT • Single adenoma • Preop sestimibi will reveal diffuse glandular involvement MEN I
Parathyroid • Autosomal dominant • Genetic testing • Found on MENIN gene • Chromosome 11q13 • Family screening • should be accomplished on 1st degree relatives • early teen years • Include serum • Calcium Fasting Insulin VIP • Glucose Pancreatic Polypeptide Prolactin • Gastrin Growth Hormone b-human Gonadotropin • Annual calcium screening should occur in 1st degree relatives MEN I
Parathyroid • There is no curative operation • Preferred corrective strategy employs 3.5 gland excision • Optional total parathyroidectomy with autotransplantation to forearm • Achieves cure > 90% of cases • Recurrent hyperparathyroidism • after autotransplantation to forearm ~ 50% recurrence • Resection of autotransplanted material • Hypoparathyroidism postop occurrence < 5% • Treated with oral supplementation MEN I
MEN I • Involves the 3 P’s • Pituitary • Parathyroid • Pancreatic islet cells MEN I
Pituitary • Occur in 40% of MEN I pts • Most commonly benign prolactin secreting adenomas • May produce • Growth hormone • ACTH • rarely nonfunctional adenomas • Presenting symptoms • Headache • Diplopia • Symptoms associated with hormone overproduction • Galactorrhea, Gynecomastia • Acromegally • Cushing’s Syndrome • thin skin/stretch marks • proximal muscle weakness • hyperglycemia MEN I
Pituitary • Bromocriptinemesylate • Dopamine agonist • First line therapy • Inhibits prolactin production • Reduces tumor bulk • Cabergoline is second line therapy for pts unable to tolerate Bromocriptinemesylate • Trans-sphenoidalhypophysectomy for medical failures • 3 months of therapy • Failure to improve prolactin levels or diplopia • Cabergoline more effective in tumor shinkage MEN I
MEN I • Involves the 3 P’s • Pituitary • Parathyroid • Pancreatic islet cells MEN I
Pancreatic islet cells • Poses most difficult clinical challenge • Pancreas is diffusely involved • Islet cell hyperplasia • Multifocal tumors • Accounts for most morbidity and mortality • Gastrinoma (Zollinger-Ellison) • Vasoactive intestinal polypeptidoma (VIPoma) • Insulinoma • Glucagonoma • Somatostatinoma • 90% found in gastrinoma triangle and are malignant • Junction of cystic duct and CBD • Junction of 2nd and 3rd portions of duodenum • Junction of body and neck of pancreas • Therapy directed at palliation of symptoms and the malignant process MEN I
Junction of cystic duct and CBD Junction of 2nd and 3rd portions of duodenum Junction of body and neck of pancreas Gastrinoma Triangle
MEN I • Involves the 3 P’s • Pituitary • Parathyroid • Pancreatic islet cells • MEN II • MEN II-A • Medullary carcinoma of thyroid • Pheochromocytoma • Parathyroid hyperplasia • MEN II-B • Medullary carcinoma of thyroid • Pheochromocytoma • Ganglioneuromatosis (mucosal neuromas) • Marfanoidhabitus MEN I/MEN II
MEN II • MEN II-A • Medullary carcinoma of thyroid • Pheochromocytoma • Parathyroid hyperplasia MEN II-A
Medullary carcinoma of thyroid • Present in all pts • Autosomal dominant syndrome • Gain-of-function mutation in RET proto-oncogene • Prophylactic thyroidectomy indicated for all RET-mutation carriers upon discovery1 • Greatest survival benefit if thyroidectomy completed < 5 yoa for MEN II-A2 • Age specific progression from C cell hyperplasia to medullary thyroid cancer to nodal metastasis • After primary resection – recurrence in over 50% pts • No recurrence/nodal metastasis in pts < 14 yoa • Re-operation for locally recurrent disease • No accepted adjuvant therapy for metastatic disease • 1Machens et al. N Engl J Med 2003;349:1517 • 2Brandi ML, et al. J ClinEdnocrinolMetab 2001;86:5658 MEN II-A
MEN II • MEN II-A • Medullary carcinoma of thyroid • Pheochromocytoma • Parathyroid hyperplasia MEN II-A
Pheochromocytoma • Present in 40-50% of pts • Biochemical testing recommended in all: • Medullary thyroid cancer pts • MEN II pts • Includes • 24 hour urinary catecholamines/metanephrines/VMA • Plasma metanephrines • Discontinue antihypertensives 24 hours prior to collection MEN II-A
MEN II • MEN II-A • Medullary carcinoma of thyroid • Pheochromocytoma • Parathyroid hyperplasia MEN II-A
Parathyroid hyperplasia • Arises in 25-35% of pts • Similar to MEN I • Diffuse/multiglandular • Metachronous development of multiple adenomas • Preferred corrective strategy employs 3.5 gland excision MEN II-A
MEN I • Involves the 3 P’s • Pituitary • Parathyroid • Pancreatic islet cells • MEN II • MEN II-A • Medullary carcinoma of thyroid • Pheochromocytoma • Parathyroid hyperplasia • MEN II-B • Medullary carcinoma of thyroid • Pheochromocytoma • Ganglioneuromatosis (mucosal neuromas) • Marfanoidhabitus MEN I/MEN II
MEN II • MEN II-B • Medullary carcinoma of thyroid • Pheochromocytoma • Ganglioneuromatosis (mucosal neuromas) • Marfanoid habitus MEN II-B
MEN II • MEN II-B • Medullary carcinoma of thyroid • Pheochromocytoma • Ganglioneuromatosis (mucosal neuromas) • Marfanoid habitus MEN II-B
Medullary carcinoma of thyroid • Present in all pts • Autosomal dominant syndrome • Gain-of-function mutation in RET proto-oncogene • Prophylactic thyroidectomy indicated for all RET-mutation carriers upon discovery1 • Greatest survival benefit if thyroidectomy completed < 1 yoa for MEN II-B2 • Age specific progression from C cell hyperplasia to medullary thyroid cancer to nodal metastasis • After primary resection – recurrence in over 50% pts • No recurrence/nodal metastasis in pts < 14 yoa • Re-operation for locally recurrent disease • No accepted adjuvant therapy for metastatic disease • 1Machens et al. N Engl J Med 2003;349:1517 • 2Brandi ML, et al. J ClinEdnocrinolMetab 2001;86:5658 MEN II-B
MEN II • MEN II-B • Medullary carcinoma of thyroid • Pheochromocytoma • Ganglioneuromatosis (mucosal neuromas) • Marfanoid habitus MEN II-B
Pheochromocytoma • Present in 40-50% of pts • Biochemical testing recommended in all: • Medullary thyroid cancer pts • MEN II pts • Includes • 24 hour urinary catecholamines/metanephrines/VMA • Plasma metanephrines • Discontinue antihypertensives 24 hours prior to collection MEN II-A
MEN II • MEN II-B • Medullary carcinoma of thyroid • Pheochromocytoma • Ganglioneuromatosis (mucosal neuromas) • Marfanoid habitus MEN II-B
Multiple mucosal neuromas Ganglioneuromatosis (mucosal neuromas)
Multiple mucosal neuromas Ganglioneuromatosis (mucosal neuromas)
Multiple mucosal neuromas Ganglioneuromatosis (mucosal neuromas)
MEN II • MEN II-B • Medullary carcinoma of thyroid • Pheochromocytoma • Ganglioneuromatosis (mucosal neuromas) • Marfanoid habitus MEN II-B
Mild ptosis Prominent nose and lips Macrognathia MEN II-B
Prominent corneal nerves MEN II-B
Prominent lips Mucosal neuromas MEN II-B