Download
1 / 21
210 likes | 432 Views
FAISAL GHANI SIDDIQUI MBBS; FCPS; MCPS (HPE); PGD (BIOETHICS) faisal@ lumhs.edu.pk www.lumhs.edu.pk /faculties/surgery/ gsurgery /about- dr.faisalghani.html. PREAMBLE. DIFFICULTY IN SWALLOWING RESULTS FROM ANY PATHOLOGY THAT INTERFERES WITH THE NORMAL SWALLOWING MECHANISM. ORAL PHARYNGEAL

E N D
FAISAL GHANI SIDDIQUI MBBS; FCPS; MCPS (HPE); PGD (BIOETHICS) faisal@lumhs.edu.pk www.lumhs.edu.pk/faculties/surgery/gsurgery/about-dr.faisalghani.html
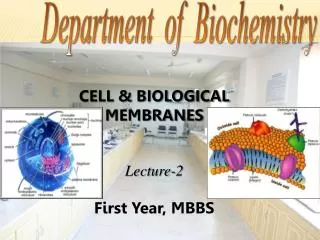
DIFFICULTY IN SWALLOWING RESULTS FROM ANY PATHOLOGY THAT INTERFERES WITH THE NORMAL SWALLOWING MECHANISM
ORAL PHARYNGEAL OESOPHAGEAL
ORAL PHASEFOOD BOLUS ROLLED BACK BY THE TONGUE INTO THE PHARYNX PHARYNGEAL PHASEFOOD PASSES THROUGH THE PHARYNX INTO THE OESOPHAGUS OESOPHAGEAL PHASEFOOD PASSES THROUGH THE OESOPHAGUS INTO THE STOMACH
HIGH (OROPHARYNGEAL)DYSPHAGIA OCCURING AT OR ABOVE CRICOPHARYNGEUS LOW (OESOPHAGEAL)DYSPHAGIA OCCURING BELOW CRICOPHARYNGEUS
HIGH (OROPHARYNGEAL) DYSPHAGIA ASSOCIATED WITH CHOKING OR COUGHING IMMEDIATELY AFTER SWALLOWING SWALLOWING SOLIDS EASIER THAN LIQUIDS
DYSPHAGIA DUE TO OESOPHAGEAL CARCINOMA SHORT DURATION (< 3 MONTHS) PROGRESSIVE ASSOCIATED WEIGHT LOSS
DYSPHAGIA DUE TO MOTILITY DISORDERS LONG HISTORY INVOLVES BOTH SOLIDS AND LIQUIDS DYSPHAGIA MAY DISAPPEAR, BEING REPLACED WITH REGURGITATION & NOCTURNAL COUGH
OFTEN UNREWARDING MOVEMENTS OF TONGUE, PALATE, & MUSCLES OF FACIAL EXPRESSION CERVICAL LYMPHADENOPATHY WEIGHT LOSS
PATIENTS WITH HIGH DYSPHAGIA WITH NO OBVIOUS NEUROLOGICAL CAUSE SHOULD BE REFERRED TO ENT SPECIALIST FLEXIBLE LARYNGOSCOPY FLEXIBLE NASOENDOSCOPY RIGID ENDOSCOPY
OESOPHAGEAL DYSPHAGIA BIOPSIES TO DIFFERENTIATE MALIGNANT & BENIGN STRICTURES THERAPEUTIC; DILATATION OF BENIGN STRICTURES / MOTILITY DISORDERS STENTING IN INOPERABLE TUMOURS
OESOPHAGEAL DYSPHAGIA Demonstrates different structural pathologies Hiatus hernia | Strictures Achalasia |Tumours
PATIENTS WITH NO STRUCTURAL ABNORMALITY ON ENDOSCOPYREQUIRE FURTHER INVESTIGATION WITH MANOMETRYTO EXCLUDE MOTILITY DISORDERS
USED FOR STAGING OF HISTOLOGICALLY PROVEN OESOPHAGO-GASTRIC CARCINOMA WALL PENETRATION LYMPH NODE INVOLVEMENT EXTRINSIC OESOPHAGEAL COMPRESSION